Muhammad Junaid Akram, Jiajin Li, Asad Nawaz, Xu Qian, Haixin Huang, Jinpeng Zhang, Zahoor Elahi, Lingjuan Liu, Bo Pan, Yuxing Yuan, Tian Jie
{"title":"LVEF 53% as a Novel Mortality Predictor in Pediatric Heart Failure: A Multicenter Biomarker-Stratified Analysis.","authors":"Muhammad Junaid Akram, Jiajin Li, Asad Nawaz, Xu Qian, Haixin Huang, Jinpeng Zhang, Zahoor Elahi, Lingjuan Liu, Bo Pan, Yuxing Yuan, Tian Jie","doi":"10.3390/diagnostics15192530","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b>: Pediatric heart failure (PHF) remains a major contributor to morbidity and mortality, yet standardized diagnostic and prognostic frameworks-particularly those leveraging left ventricular ejection fraction (LVEF)-are not well-established. This study evaluates clinical profiles, therapeutic interventions, and mortality outcomes across LVEF thresholds while identifying an optimal cutoff to refine risk stratification in PHF. <b>Methods</b>: This multicenter retrospective cohort study analyzed 1449 PHF patients (aged 1-18 years) across 30 tertiary centers (2013-2022). LVEF stratification employed conventional thresholds (50%, 55%) and an ROC-optimized cutoff (53%, derived via Youden index maximization). The primary outcome was in-hospital all-cause mortality. Multivariable logistic regression models, adjusted for clinical covariates, evaluated mortality predictors. The discriminative performance of LVEF thresholds was compared using area under the curve (AUC) analysis. <b>Results</b>: Distinct clinical profiles, etiologies, and treatments were observed across LVEF strata (50% vs. 55%; <i>p</i> < 0.05). A data-driven optimized LVEF threshold of 53% was identified for mortality prediction, demonstrating superior diagnostic accuracy with enhanced sensitivity and specificity across age groups. Multivariate analysis revealed LVEF ≥ 55% as protective (OR = 0.81, 95% CI: 0.68-0.96, <i>p</i> = 0.003), while ≥50% was non-significant (OR = 0.91, 95% CI: 0.74-1.12, <i>p</i> = 0.06). Elevated BNP (OR = 2.78, <i>p</i> < 0.001) and NT-proBNP (OR = 2.34, <i>p</i> < 0.001) strongly correlated with mortality risk. Age and sex showed no significant association with outcomes. <b>Conclusion</b>: In conclusion, an LVEF of 53% emerged as the optimal pediatric threshold for mortality prediction, outperforming conventional cutoffs of 50% and 55%. The integration of LVEF with biomarkers (BNP/NT-proBNP) provides a robust prognostic framework, underscoring the necessity for pediatric-specific LVEF criteria and multidimensional risk assessment in PHF management.</p>","PeriodicalId":11225,"journal":{"name":"Diagnostics","volume":"15 19","pages":""},"PeriodicalIF":3.3000,"publicationDate":"2025-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12524215/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diagnostics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/diagnostics15192530","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
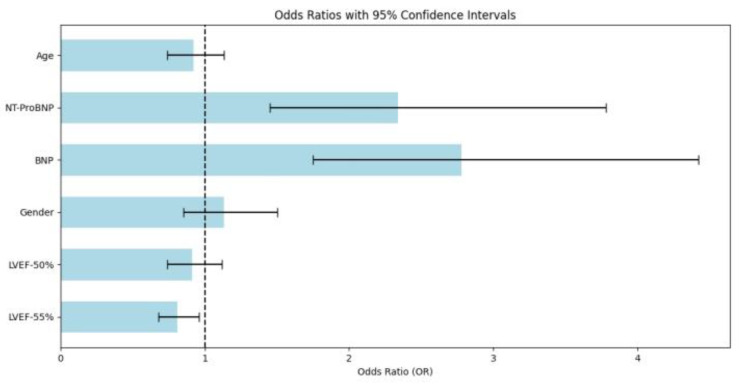
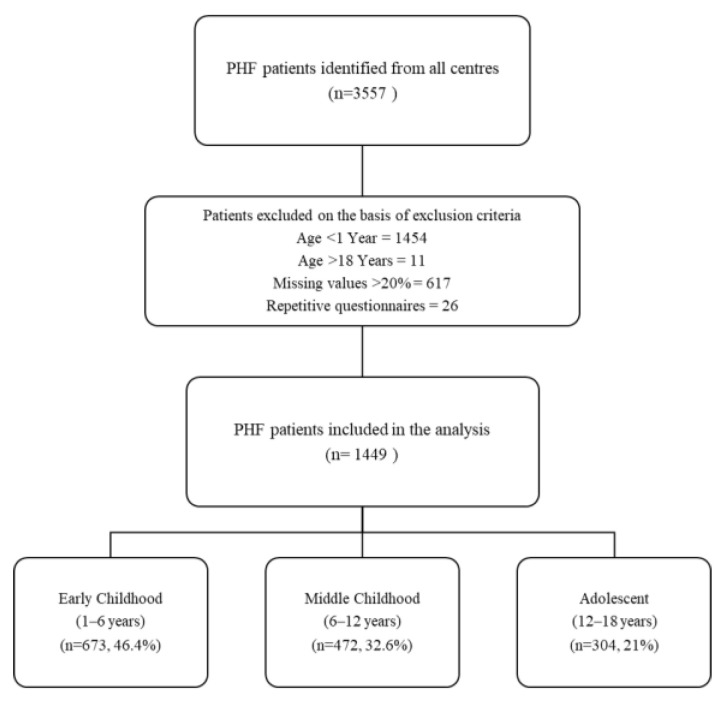
Background: Pediatric heart failure (PHF) remains a major contributor to morbidity and mortality, yet standardized diagnostic and prognostic frameworks-particularly those leveraging left ventricular ejection fraction (LVEF)-are not well-established. This study evaluates clinical profiles, therapeutic interventions, and mortality outcomes across LVEF thresholds while identifying an optimal cutoff to refine risk stratification in PHF. Methods: This multicenter retrospective cohort study analyzed 1449 PHF patients (aged 1-18 years) across 30 tertiary centers (2013-2022). LVEF stratification employed conventional thresholds (50%, 55%) and an ROC-optimized cutoff (53%, derived via Youden index maximization). The primary outcome was in-hospital all-cause mortality. Multivariable logistic regression models, adjusted for clinical covariates, evaluated mortality predictors. The discriminative performance of LVEF thresholds was compared using area under the curve (AUC) analysis. Results: Distinct clinical profiles, etiologies, and treatments were observed across LVEF strata (50% vs. 55%; p < 0.05). A data-driven optimized LVEF threshold of 53% was identified for mortality prediction, demonstrating superior diagnostic accuracy with enhanced sensitivity and specificity across age groups. Multivariate analysis revealed LVEF ≥ 55% as protective (OR = 0.81, 95% CI: 0.68-0.96, p = 0.003), while ≥50% was non-significant (OR = 0.91, 95% CI: 0.74-1.12, p = 0.06). Elevated BNP (OR = 2.78, p < 0.001) and NT-proBNP (OR = 2.34, p < 0.001) strongly correlated with mortality risk. Age and sex showed no significant association with outcomes. Conclusion: In conclusion, an LVEF of 53% emerged as the optimal pediatric threshold for mortality prediction, outperforming conventional cutoffs of 50% and 55%. The integration of LVEF with biomarkers (BNP/NT-proBNP) provides a robust prognostic framework, underscoring the necessity for pediatric-specific LVEF criteria and multidimensional risk assessment in PHF management.
DiagnosticsBiochemistry, Genetics and Molecular Biology-Clinical Biochemistry
CiteScore
4.70
自引率
8.30%
发文量
2699
审稿时长
19.64 days
期刊介绍:
Diagnostics (ISSN 2075-4418) is an international scholarly open access journal on medical diagnostics. It publishes original research articles, reviews, communications and short notes on the research and development of medical diagnostics. There is no restriction on the length of the papers. Our aim is to encourage scientists to publish their experimental and theoretical research in as much detail as possible. Full experimental and/or methodological details must be provided for research articles.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


