{"title":"When the Pupils Lie: Unmasking an Unnoticed High Spinal Anesthesia During Orthopedic Surgery.","authors":"Kartik Sonawane, Sumeet Patil, Satheesh Kumar, Tuhin Mistry, Palanichamy Gurumoorthi, Chelliah Sekar","doi":"10.7759/cureus.94047","DOIUrl":null,"url":null,"abstract":"<p><p>High spinal anesthesia is a rare but potentially serious complication of neuraxial techniques. Unlike total spinal anesthesia, which typically presents dramatically with profound cardiovascular collapse, high spinal anesthesia may evolve more insidiously and manifest primarily with neurological signs. We report the case of a 23-year-old polytrauma patient undergoing femur and tibia fixation under combined spinal-epidural anesthesia (CSEA) who developed sudden unresponsiveness with fixed, dilated pupils shortly after femoral canal reaming. An epidural top-up of 10 mL 0.25% bupivacaine was administered 2.5 hours into surgery, with neurological deterioration occurring approximately 30 minutes later. Despite this alarming presentation, his hemodynamics and spontaneous ventilation remained stable, and he regained consciousness within 30 minutes without airway intervention. Postoperative evaluation revealed intrathecal migration of the epidural catheter, with the block extending above T2 and causing bilateral upper limb weakness. Arterial blood gas analysis demonstrated metabolic and respiratory acidosis, reflecting transient hypoventilation. This case illustrates how an unnoticed high spinal anesthesia can mimic catastrophic neurological or embolic events yet remain fully reversible. It underscores the importance of careful catheter management, structured differential diagnosis, and preparedness for airway intervention.</p>","PeriodicalId":93960,"journal":{"name":"Cureus","volume":"17 10","pages":"e94047"},"PeriodicalIF":1.3000,"publicationDate":"2025-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12507387/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cureus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7759/cureus.94047","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
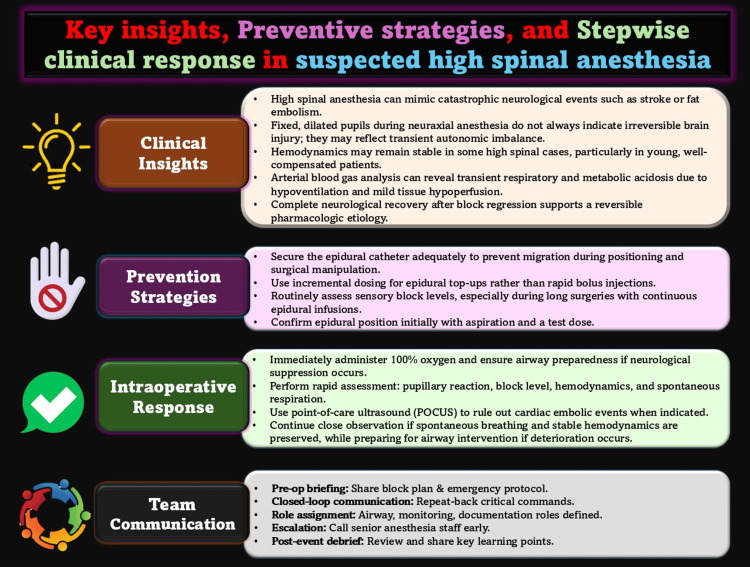
High spinal anesthesia is a rare but potentially serious complication of neuraxial techniques. Unlike total spinal anesthesia, which typically presents dramatically with profound cardiovascular collapse, high spinal anesthesia may evolve more insidiously and manifest primarily with neurological signs. We report the case of a 23-year-old polytrauma patient undergoing femur and tibia fixation under combined spinal-epidural anesthesia (CSEA) who developed sudden unresponsiveness with fixed, dilated pupils shortly after femoral canal reaming. An epidural top-up of 10 mL 0.25% bupivacaine was administered 2.5 hours into surgery, with neurological deterioration occurring approximately 30 minutes later. Despite this alarming presentation, his hemodynamics and spontaneous ventilation remained stable, and he regained consciousness within 30 minutes without airway intervention. Postoperative evaluation revealed intrathecal migration of the epidural catheter, with the block extending above T2 and causing bilateral upper limb weakness. Arterial blood gas analysis demonstrated metabolic and respiratory acidosis, reflecting transient hypoventilation. This case illustrates how an unnoticed high spinal anesthesia can mimic catastrophic neurological or embolic events yet remain fully reversible. It underscores the importance of careful catheter management, structured differential diagnosis, and preparedness for airway intervention.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


