Ola Mounir, Ahmed Sedky, Omar M Mohafez, Sahar A Elsayed
{"title":"Cystatin D as a biomarker for rheumatoid arthritis: relation to disease activity and joint damage.","authors":"Ola Mounir, Ahmed Sedky, Omar M Mohafez, Sahar A Elsayed","doi":"10.5114/reum/199871","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Rheumatoid arthritis (RA) is a multisystem autoimmune disorder. Autoantibody levels in the serum of RA patients can guide the diagnosis and treatment. Cystatin D is a known inhibitor of cathepsins involved in RA pathogenesis. We aimed to determine the value of cystatin D in RA patients and to explore the relation between cystatin D serum level and disease activity and joint damage.</p><p><strong>Material and methods: </strong>Seventy adult RA patients and 40 sex- and age-matched healthy controls were included in this study. The patients' clinical, demographic, and rheumatologic data were recorded. Disease activity was measured using the Disease Activity Score in 28 joints (DAS28). Laboratory tests comprising complete blood count, erythrocyte sedimentation rate (ESR), C-reactive protein, serum creatinine, alanine aminotransferase, aspartate aminotransferase, rheumatoid factor, anti-citrullinated protein antibodies, and serum cystatin D were measured. In addition, we used the modified Larsen score to evaluate radiologic joint damage.</p><p><strong>Results: </strong>Cystatin D was elevated in RA patients compared to the controls and was negatively correlated with ESR, DAS28, and Larsen scores. At a cutoff value of 3.64 ng/ml, cystatin D could differentiate RA patients from healthy controls with 81.4% sensitivity and 75% specificity (<i>p</i> < 0.001). At a cutoff value of 5.22 ng/ml, cystatin D showed a significant value (<i>p</i> = 0.007) for differentiating active RA patients from those in remission, with 69.2% sensitivity and 78.9% specificity.</p><p><strong>Conclusions: </strong>Cystatin D may be a valuable marker for RA with good sensitivity and specificity. Moreover, its negative correlation with the DAS28 and the Larsen score suggests that it may be a marker adding to the DAS28 for the follow-up of disease activity and prediction of radiological joint damage. However, further studies with large sample sizes and long follow-up periods are required.</p>","PeriodicalId":21312,"journal":{"name":"Reumatologia","volume":"63 4","pages":"222-228"},"PeriodicalIF":1.7000,"publicationDate":"2025-08-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12503156/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reumatologia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/reum/199871","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Rheumatoid arthritis (RA) is a multisystem autoimmune disorder. Autoantibody levels in the serum of RA patients can guide the diagnosis and treatment. Cystatin D is a known inhibitor of cathepsins involved in RA pathogenesis. We aimed to determine the value of cystatin D in RA patients and to explore the relation between cystatin D serum level and disease activity and joint damage.
Material and methods: Seventy adult RA patients and 40 sex- and age-matched healthy controls were included in this study. The patients' clinical, demographic, and rheumatologic data were recorded. Disease activity was measured using the Disease Activity Score in 28 joints (DAS28). Laboratory tests comprising complete blood count, erythrocyte sedimentation rate (ESR), C-reactive protein, serum creatinine, alanine aminotransferase, aspartate aminotransferase, rheumatoid factor, anti-citrullinated protein antibodies, and serum cystatin D were measured. In addition, we used the modified Larsen score to evaluate radiologic joint damage.
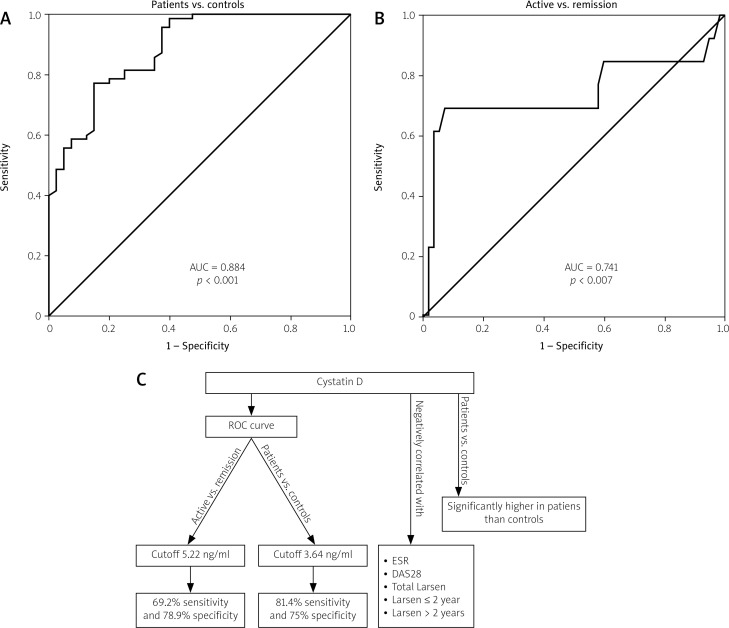
Results: Cystatin D was elevated in RA patients compared to the controls and was negatively correlated with ESR, DAS28, and Larsen scores. At a cutoff value of 3.64 ng/ml, cystatin D could differentiate RA patients from healthy controls with 81.4% sensitivity and 75% specificity (p < 0.001). At a cutoff value of 5.22 ng/ml, cystatin D showed a significant value (p = 0.007) for differentiating active RA patients from those in remission, with 69.2% sensitivity and 78.9% specificity.
Conclusions: Cystatin D may be a valuable marker for RA with good sensitivity and specificity. Moreover, its negative correlation with the DAS28 and the Larsen score suggests that it may be a marker adding to the DAS28 for the follow-up of disease activity and prediction of radiological joint damage. However, further studies with large sample sizes and long follow-up periods are required.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


