{"title":"Epicardial adipose tissue thickness on transthoracic echocardiography predicts 2-year incident atrial fibrillation in elderly hypertensive patients.","authors":"Mintao Ma, Xiaoye Zheng, Xiaojuan Wu, Qing Xie","doi":"10.3389/fcvm.2025.1650423","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Epicardial adipose tissue (EAT) promotes atrial remodeling, yet prospective data on whether a single transthoracic-echocardiographic measurement of EAT can identify elderly hypertensive patients at short-term risk of atrial fibrillation (AF) are limited.</p><p><strong>Methods: </strong>In this single-center cohort study (March 2021-June 2024), 460 hypertensive adults aged ≥65 years in sinus rhythm were enrolled; epicardial adipose tissue thickness was measured on the right-ventricular free wall, and participants underwent intensive multimodal rhythm surveillance for 24 months. Cox models were adjusted for age, body mass index, systolic blood pressure, diabetes, left-atrial (LA) volume index, and β-blocker use; performance was optimism-corrected with 200 bootstraps.</p><p><strong>Results: </strong>During 902 person-years of follow-up, 55 participants (12.0%; 6.1 events per 100 person-years) developed incident AF. Baseline EAT was greater in cases than in controls (7.9 ± 1.4 vs. 5.7 ± 1.2 mm; <i>p</i> < 0.001). Each 1 mm increase in EAT independently conferred a 62% higher AF hazard [hazard ratio (HR): 1.62, 95% CI: 1.29-2.04]; the optimism-corrected HR was 1.56. The findings were consistent in those with treated obstructive sleep apnea (OSA) (HR: 1.60) and in those without OSA (HR: 1.59; interaction <i>p</i> = 0.93) and after additional adjustment for high-sensitivity C-reactive protein (HR: 1.55 in 410 participants with biomarker data). Adding continuous EAT to a clinical model improved the C-index from 0.74 to 0.79 (optimism-corrected 0.78), reduced the Akaike information criterion by 16 points, and yielded a continuous net reclassification improvement of 0.25 (95% CI: 0.09-0.39) and an integrated discrimination improvement gain of 0.05. Time-specific area under the receiver-operating-characteristic curves (AUCs) remained ≥0.76 and calibration was preserved (Grønnesby-Borgan <i>p</i> ≥ 0.60). A receiver-operating-characteristic analysis identified 6.5 mm as the optimal EAT threshold (80% sensitivity, 68% specificity); 24-month AF incidence rate was 24.7% above vs. 4.1% below this cut point (log-rank <i>p</i> < 0.001). The EAT-AF association was robust in Fine-Gray competing-risk models and consistent across sex, obesity, diabetes, and LA-size strata (all interaction <i>p</i> > 0.20).</p><p><strong>Conclusions: </strong>Echocardiographic EAT thickness is a reproducible and incrementally informative predictor of 2-year incident AF in elderly hypertensive patients. Incorporating this simple metric into routine scans could refine risk stratification and guide targeted rhythm surveillance.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"12 ","pages":"1650423"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12500569/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2025.1650423","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Epicardial adipose tissue (EAT) promotes atrial remodeling, yet prospective data on whether a single transthoracic-echocardiographic measurement of EAT can identify elderly hypertensive patients at short-term risk of atrial fibrillation (AF) are limited.
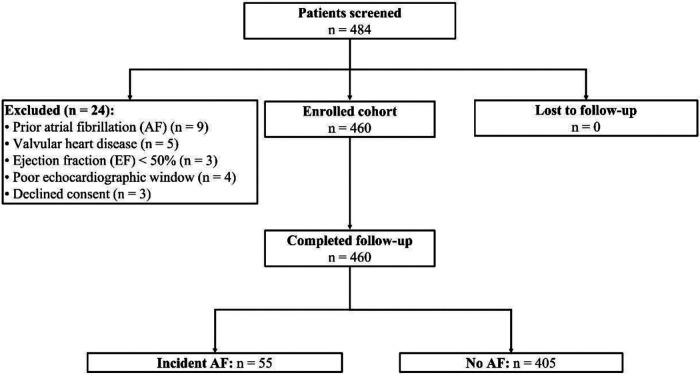
Methods: In this single-center cohort study (March 2021-June 2024), 460 hypertensive adults aged ≥65 years in sinus rhythm were enrolled; epicardial adipose tissue thickness was measured on the right-ventricular free wall, and participants underwent intensive multimodal rhythm surveillance for 24 months. Cox models were adjusted for age, body mass index, systolic blood pressure, diabetes, left-atrial (LA) volume index, and β-blocker use; performance was optimism-corrected with 200 bootstraps.
Results: During 902 person-years of follow-up, 55 participants (12.0%; 6.1 events per 100 person-years) developed incident AF. Baseline EAT was greater in cases than in controls (7.9 ± 1.4 vs. 5.7 ± 1.2 mm; p < 0.001). Each 1 mm increase in EAT independently conferred a 62% higher AF hazard [hazard ratio (HR): 1.62, 95% CI: 1.29-2.04]; the optimism-corrected HR was 1.56. The findings were consistent in those with treated obstructive sleep apnea (OSA) (HR: 1.60) and in those without OSA (HR: 1.59; interaction p = 0.93) and after additional adjustment for high-sensitivity C-reactive protein (HR: 1.55 in 410 participants with biomarker data). Adding continuous EAT to a clinical model improved the C-index from 0.74 to 0.79 (optimism-corrected 0.78), reduced the Akaike information criterion by 16 points, and yielded a continuous net reclassification improvement of 0.25 (95% CI: 0.09-0.39) and an integrated discrimination improvement gain of 0.05. Time-specific area under the receiver-operating-characteristic curves (AUCs) remained ≥0.76 and calibration was preserved (Grønnesby-Borgan p ≥ 0.60). A receiver-operating-characteristic analysis identified 6.5 mm as the optimal EAT threshold (80% sensitivity, 68% specificity); 24-month AF incidence rate was 24.7% above vs. 4.1% below this cut point (log-rank p < 0.001). The EAT-AF association was robust in Fine-Gray competing-risk models and consistent across sex, obesity, diabetes, and LA-size strata (all interaction p > 0.20).
Conclusions: Echocardiographic EAT thickness is a reproducible and incrementally informative predictor of 2-year incident AF in elderly hypertensive patients. Incorporating this simple metric into routine scans could refine risk stratification and guide targeted rhythm surveillance.
背景:心外膜脂肪组织(EAT)促进心房重构,然而单次经胸超声心动图测量EAT是否能识别有房颤(AF)短期风险的老年高血压患者的前瞻性数据有限。方法:在这项单中心队列研究中(2021年3月- 2024年6月),纳入460名年龄≥65岁的高血压成人;在右心室游离壁上测量心外膜脂肪组织厚度,并对参与者进行24个月的多模式节律监测。对Cox模型进行年龄、体重指数、收缩压、糖尿病、左房(LA)容积指数和β受体阻滞剂使用等因素调整;表现是乐观修正了200次引导。结果:在902人-年的随访期间,55名参与者(12.0%,每100人-年6.1次事件)发生了AF。病例的基线EAT高于对照组(7.9±1.4 vs. 5.7±1.2 mm; p p = 0.93),在额外调整高敏感性c反应蛋白后(410名有生物标志物数据的参与者的HR: 1.55)。在临床模型中加入连续EAT后,c指数从0.74提高到0.79(乐观修正0.78),赤池信息标准降低了16点,连续净重分类改善为0.25 (95% CI: 0.09-0.39),综合判别改善增益为0.05。受试者工作特征曲线下的时间特异面积(auc)保持≥0.76,并保持校准(Grønnesby-Borgan p≥0.60)。接受者工作特征分析确定6.5 mm为最佳EAT阈值(80%敏感性,68%特异性);24个月房颤发病率高于该切点24.7%,低于该切点4.1% (log-rank p p > 0.20)。结论:超声心动图EAT厚度是老年高血压患者2年内发生房颤的一个可重复和增量信息预测指标。将这一简单的指标纳入常规扫描可以完善风险分层,并指导有针对性的心律监测。
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


