{"title":"Assessing the consistency of mass spectrometry, a clinical-laboratory model, and immunohistochemistry in amyloid subtyping: a Brazilian experience.","authors":"Roberta Shcolnik Szor, Jussara Bianchi Castelli, Rodrigo Andrade Schuch, Valdemir Melechco Carvalho, Vanderson Rocha","doi":"10.1186/s12014-025-09546-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Systemic amyloidosis is a potentially fatal protein misfolding disorder usually underdiagnosed in low- and middle-income countries, where limited awareness and restricted access to diagnostic tools contribute to prolonged diagnostic journeys and delayed diagnoses. Accurate identification of the precursor protein is essential but remains a challenge, particularly in resource-limited settings. This study aimed to perform mass spectrometry (MS) for amyloid subtyping and to use it as the reference method to evaluate the consistency of a clinical-laboratory model (CLM) and immunohistochemistry (IHC) in determining the amyloid subtype.</p><p><strong>Methods: </strong>In this retrospective, observational, single-center study, MS was performed on tissue biopsies from patients diagnosed with systemic amyloidosis between 2009 and 2018 at a public university hospital in Brazil. An IHC panel of four antibodies (anti-kappa, -lambda, -serum amyloid A, -transthyretin) was performed on samples with sufficient material. Review of medical records assessed the amyloid subtype determined by the clinical-laboratory model (CLM), which was based on clinical presentation, laboratory and imaging data, genetic testing, and pathological findings available at the time of the initial diagnosis.</p><p><strong>Results: </strong>From 127 patients, 48 were excluded due to unavailable biopsies or insufficient material for MS analysis. The final cohort consisted of 79 patients, 61% male, with a median age of 61 years. Biopsies from 13 different tissues were analyzed by MS, revealing the following amyloid subtypes: AL (56%), ATTR (25%), AA (6%), AFib (3%), AH (1%). Seven cases (9%) remained inconclusive. IHC correctly subtyped amyloid in 28% of cases but failed in 66%. In 80% of patients the CLM correctly identified the amyloid subtype. However, it generated incorrect typing leading to inappropriate treatments.</p><p><strong>Conclusion: </strong>The consistency analysis between the CLM, IHC and MS demonstrated the superiority of MS in amyloid subtyping from tissue biopsies. While the CLM failed in 20% of cases and resulted in inappropriate treatments due to false-positive results, IHC showed very limited diagnostic performance, contrasting with results from reference centers, with less than one-third of cases correctly classified. These findings reinforce the role of MS as a more accurate and cost-competitive method for amyloid subtyping in middle-income countries.</p>","PeriodicalId":10468,"journal":{"name":"Clinical proteomics","volume":"22 1","pages":"35"},"PeriodicalIF":3.3000,"publicationDate":"2025-10-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12505685/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical proteomics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12014-025-09546-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"BIOCHEMICAL RESEARCH METHODS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Systemic amyloidosis is a potentially fatal protein misfolding disorder usually underdiagnosed in low- and middle-income countries, where limited awareness and restricted access to diagnostic tools contribute to prolonged diagnostic journeys and delayed diagnoses. Accurate identification of the precursor protein is essential but remains a challenge, particularly in resource-limited settings. This study aimed to perform mass spectrometry (MS) for amyloid subtyping and to use it as the reference method to evaluate the consistency of a clinical-laboratory model (CLM) and immunohistochemistry (IHC) in determining the amyloid subtype.
Methods: In this retrospective, observational, single-center study, MS was performed on tissue biopsies from patients diagnosed with systemic amyloidosis between 2009 and 2018 at a public university hospital in Brazil. An IHC panel of four antibodies (anti-kappa, -lambda, -serum amyloid A, -transthyretin) was performed on samples with sufficient material. Review of medical records assessed the amyloid subtype determined by the clinical-laboratory model (CLM), which was based on clinical presentation, laboratory and imaging data, genetic testing, and pathological findings available at the time of the initial diagnosis.
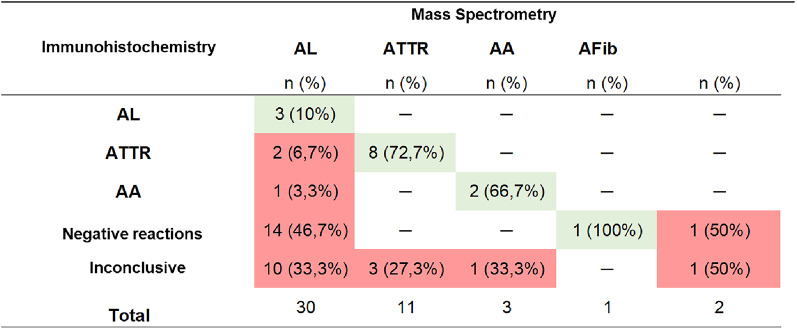
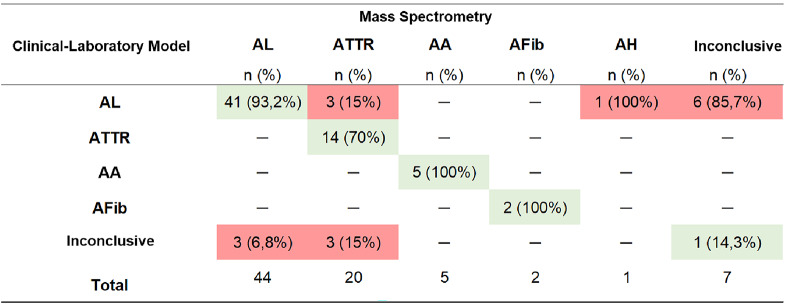
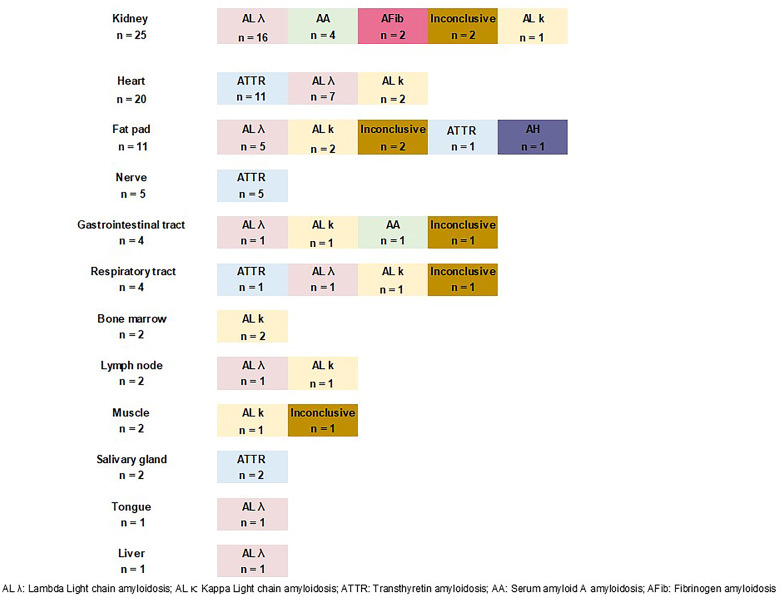
Results: From 127 patients, 48 were excluded due to unavailable biopsies or insufficient material for MS analysis. The final cohort consisted of 79 patients, 61% male, with a median age of 61 years. Biopsies from 13 different tissues were analyzed by MS, revealing the following amyloid subtypes: AL (56%), ATTR (25%), AA (6%), AFib (3%), AH (1%). Seven cases (9%) remained inconclusive. IHC correctly subtyped amyloid in 28% of cases but failed in 66%. In 80% of patients the CLM correctly identified the amyloid subtype. However, it generated incorrect typing leading to inappropriate treatments.
Conclusion: The consistency analysis between the CLM, IHC and MS demonstrated the superiority of MS in amyloid subtyping from tissue biopsies. While the CLM failed in 20% of cases and resulted in inappropriate treatments due to false-positive results, IHC showed very limited diagnostic performance, contrasting with results from reference centers, with less than one-third of cases correctly classified. These findings reinforce the role of MS as a more accurate and cost-competitive method for amyloid subtyping in middle-income countries.
期刊介绍:
Clinical Proteomics encompasses all aspects of translational proteomics. Special emphasis will be placed on the application of proteomic technology to all aspects of clinical research and molecular medicine. The journal is committed to rapid scientific review and timely publication of submitted manuscripts.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


