{"title":"Late-onset esophagogastric anastomotic fistula managed without continuous fasting: a case report.","authors":"Yuhui Gong, Yu Zhang, Haitao Ma, Wei Jiang, Jiangjiang Liu, Yunteng Kang, Jialiang Liu, Xiaojun Yu","doi":"10.1093/jscr/rjaf796","DOIUrl":null,"url":null,"abstract":"<p><p>Esophagogastric anastomotic fistula is a common complication following esophageal cancer surgery, typically occurring within the first postoperative week. Conventional management requires prolonged fasting until complete fistula closure, which significantly impacts patient quality of life. We present a case of a male who developed an esophagogastric anastomotic fistula 2 months postoperatively, complicated by a concurrent gastrobronchial fistula. Endoscopic evaluation revealed persistent gastric wall defects at the fistula site. As the disease progressed, thickened visceral pleura formed dense adhesions with the damaged gastric tissue, effectively sealing the defect and preventing digestive fluid leakage into the thoracic cavity. By promptly promoting gastric emptying and reducing gastric acid secretion, the patient resumed oral intake without developing severe infections or complications.</p>","PeriodicalId":47321,"journal":{"name":"Journal of Surgical Case Reports","volume":"2025 10","pages":"rjaf796"},"PeriodicalIF":0.5000,"publicationDate":"2025-10-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12499916/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jscr/rjaf796","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/10/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
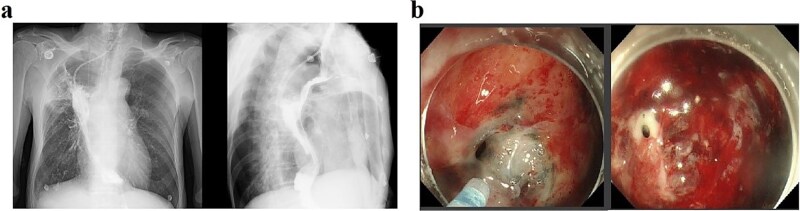
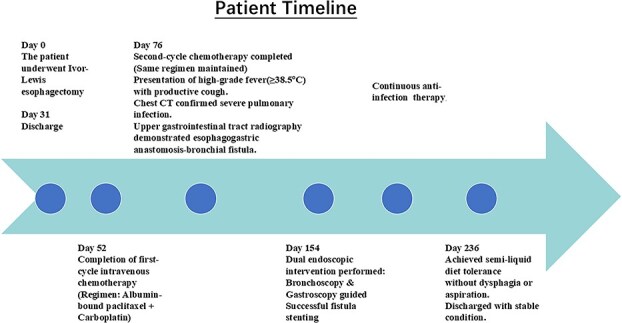
Esophagogastric anastomotic fistula is a common complication following esophageal cancer surgery, typically occurring within the first postoperative week. Conventional management requires prolonged fasting until complete fistula closure, which significantly impacts patient quality of life. We present a case of a male who developed an esophagogastric anastomotic fistula 2 months postoperatively, complicated by a concurrent gastrobronchial fistula. Endoscopic evaluation revealed persistent gastric wall defects at the fistula site. As the disease progressed, thickened visceral pleura formed dense adhesions with the damaged gastric tissue, effectively sealing the defect and preventing digestive fluid leakage into the thoracic cavity. By promptly promoting gastric emptying and reducing gastric acid secretion, the patient resumed oral intake without developing severe infections or complications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


