{"title":"Preoperative coronal imbalance in degenerative scoliosis: a study on coronal and sagittal spinal-pelvic parameters--a retrospective study.","authors":"Mei-Fang Wu, Yu-Sheng Bao, Hao Zhang, Yu-Zhi Ning, Zan Chen, Li-Peng Zheng, Fei Lei, Da-Xiong Feng","doi":"10.1186/s12891-025-09197-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To investigate the relationship between spinal-pelvic parameters in the coronal and sagittal planes and preoperative coronal imbalance (CIB) in degenerative scoliosis, aiming to prevent preoperative CIB and restore coronal balance(CB) for improved surgical outcomes.</p><p><strong>Methods: </strong>From May 2018 to May 2024, adult patients who underwent full-length spine imaging, were analyzed at the Southwest Medical University Affiliated Hospital. The inclusion criteria were: (1) availability of clear full-length spinal images in the coronal and sagittal planes that allowed for measurement of relevant parameters; (2) complete demographic information; (3) a major curve angle greater than 10°; and (4) skeletal maturity. Exclusion criteria were as follows : (1) history of previous spinal surgery; (2) pre-existing spinal or pelvic deformities; (3) history of trauma to the spine or pelvis; and (4) history of spinal infectious disease.A total of 162 cases were collected based on the inclusion and exclusion criteria.The general and imaging data of 162 patients were collected. These included the major curve (MC), fractional curve (FC), L5 tilt angle (L5TA), coronal pelvic inclination (CPI), apical vertebra translation (AVT), the number of vertebrae in the primary curve, apical vertebral rotation (AVR), sacral slope (SS), lumbar lordosis (LL), pelvic incidence (PI), pelvic tilt (PT), and sagittal vertical axis (SVA). Pearson correlation analysis and linear regression were employed to assess the relationship of each parameter with preoperative coronal balance distance (CBD). CBD was then converted to a binary variable (Patients with a CBD less than 3.0 cm were categorized into the CB group, while those with a CBD of 3.0 cm or greater were placed in the CIB group.). Univariate screening, multivariate logistic regression, and receiver operating characteristic (ROC) curve analysis were conducted to identify associations between preoperative CIB and the specified parameters.A total of 162 patients were classified into three groups based on the classification criteria of the Gulou Hospital: Type A (120 cases), Type B (25 cases), and Type C (17 cases). The differences in imaging data among the three groups were compared.</p><p><strong>Results: </strong>Pearson analysis demonstrated that L5TA, CPI, number of vertebrae in the primary curve, LL, SS, and SVA were correlated with preoperative CBD (p < 0.05). Moreover, further linear regression indicated that merely L5TA (R² = 0.204, p < 0.05), CPI (R² = 0.128, p < 0.05), and SVA (R² = 0.172, p < 0.05) were substantially associated with preoperative CBD, despite the fact that the relationship was not strictly linear. Multivariate logistic regression and ROC curve analysis revealed that age < 60.5 years was a protective factor against preoperative CIB, while preoperative L5TA > 5.75°, CPI > 3.55°, and SVA > 5.305 cm were risk factors for preoperative CIB. Among the 162 patients, 120 were classified as Type A, 25 as Type B, and 17 as Type C. Significant differences in age and L5TA were observed between the A and C groups. CBD, CPI, and SVA exhibited statistically significant differences between the A group and both the B and C groups, whereas no significant difference was found between the B and C groups.</p><p><strong>Conclusion: </strong>Preoperative L5TA is an independent risk factor for preoperative CIB. When the preoperative C7PL is located on the convex side of the major curve, L5 tilt becomes more pronounced. In the surgical treatment of DS, leveling the L5 vertebra can help reduce the incidence of postoperative CIB. Patients with degenerative scoliosis (DS) under 60.5 years of age might reduce CIB incidence through enhanced paraspinal muscle strength. Additionally, imbalances in CPI and SVA may contribute to preoperative CIB, and pelvic and sagittal alignment maintenance may offer spinal support essential for preserving coronal balance.</p>","PeriodicalId":9189,"journal":{"name":"BMC Musculoskeletal Disorders","volume":"26 1","pages":"925"},"PeriodicalIF":2.4000,"publicationDate":"2025-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12506023/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Musculoskeletal Disorders","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12891-025-09197-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To investigate the relationship between spinal-pelvic parameters in the coronal and sagittal planes and preoperative coronal imbalance (CIB) in degenerative scoliosis, aiming to prevent preoperative CIB and restore coronal balance(CB) for improved surgical outcomes.
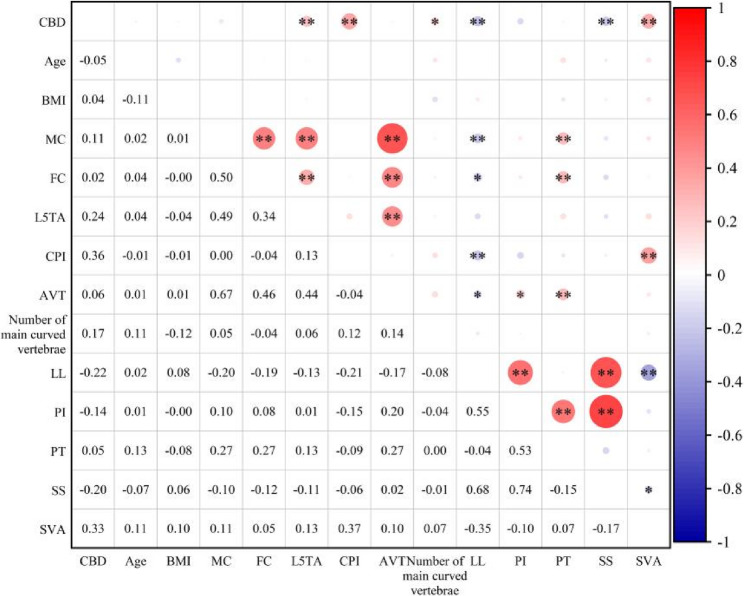
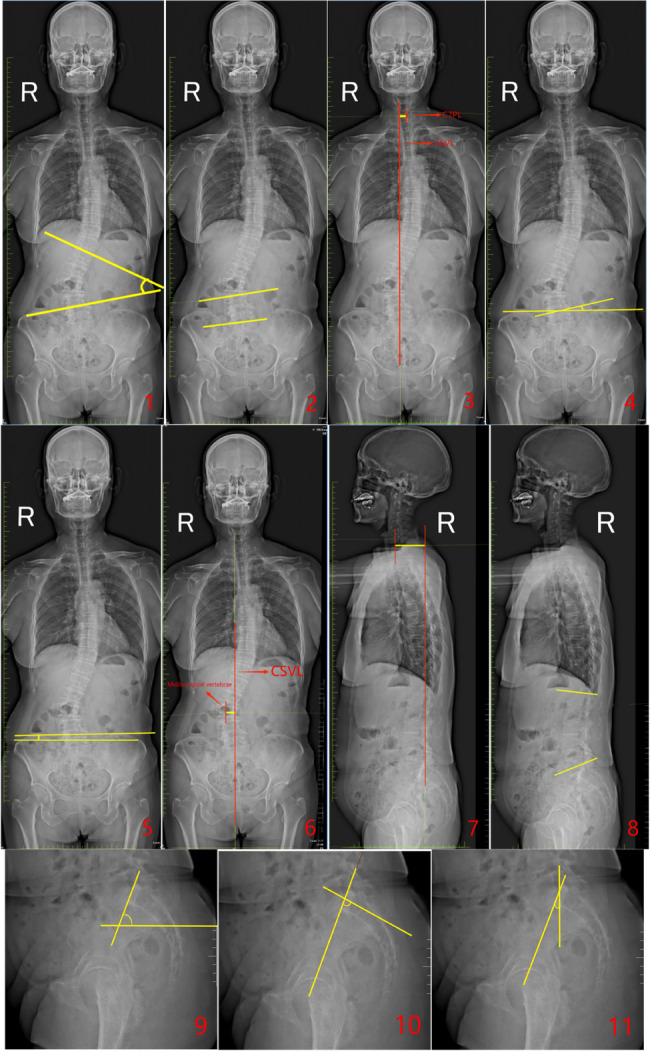
Methods: From May 2018 to May 2024, adult patients who underwent full-length spine imaging, were analyzed at the Southwest Medical University Affiliated Hospital. The inclusion criteria were: (1) availability of clear full-length spinal images in the coronal and sagittal planes that allowed for measurement of relevant parameters; (2) complete demographic information; (3) a major curve angle greater than 10°; and (4) skeletal maturity. Exclusion criteria were as follows : (1) history of previous spinal surgery; (2) pre-existing spinal or pelvic deformities; (3) history of trauma to the spine or pelvis; and (4) history of spinal infectious disease.A total of 162 cases were collected based on the inclusion and exclusion criteria.The general and imaging data of 162 patients were collected. These included the major curve (MC), fractional curve (FC), L5 tilt angle (L5TA), coronal pelvic inclination (CPI), apical vertebra translation (AVT), the number of vertebrae in the primary curve, apical vertebral rotation (AVR), sacral slope (SS), lumbar lordosis (LL), pelvic incidence (PI), pelvic tilt (PT), and sagittal vertical axis (SVA). Pearson correlation analysis and linear regression were employed to assess the relationship of each parameter with preoperative coronal balance distance (CBD). CBD was then converted to a binary variable (Patients with a CBD less than 3.0 cm were categorized into the CB group, while those with a CBD of 3.0 cm or greater were placed in the CIB group.). Univariate screening, multivariate logistic regression, and receiver operating characteristic (ROC) curve analysis were conducted to identify associations between preoperative CIB and the specified parameters.A total of 162 patients were classified into three groups based on the classification criteria of the Gulou Hospital: Type A (120 cases), Type B (25 cases), and Type C (17 cases). The differences in imaging data among the three groups were compared.
Results: Pearson analysis demonstrated that L5TA, CPI, number of vertebrae in the primary curve, LL, SS, and SVA were correlated with preoperative CBD (p < 0.05). Moreover, further linear regression indicated that merely L5TA (R² = 0.204, p < 0.05), CPI (R² = 0.128, p < 0.05), and SVA (R² = 0.172, p < 0.05) were substantially associated with preoperative CBD, despite the fact that the relationship was not strictly linear. Multivariate logistic regression and ROC curve analysis revealed that age < 60.5 years was a protective factor against preoperative CIB, while preoperative L5TA > 5.75°, CPI > 3.55°, and SVA > 5.305 cm were risk factors for preoperative CIB. Among the 162 patients, 120 were classified as Type A, 25 as Type B, and 17 as Type C. Significant differences in age and L5TA were observed between the A and C groups. CBD, CPI, and SVA exhibited statistically significant differences between the A group and both the B and C groups, whereas no significant difference was found between the B and C groups.
Conclusion: Preoperative L5TA is an independent risk factor for preoperative CIB. When the preoperative C7PL is located on the convex side of the major curve, L5 tilt becomes more pronounced. In the surgical treatment of DS, leveling the L5 vertebra can help reduce the incidence of postoperative CIB. Patients with degenerative scoliosis (DS) under 60.5 years of age might reduce CIB incidence through enhanced paraspinal muscle strength. Additionally, imbalances in CPI and SVA may contribute to preoperative CIB, and pelvic and sagittal alignment maintenance may offer spinal support essential for preserving coronal balance.
期刊介绍:
BMC Musculoskeletal Disorders is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of musculoskeletal disorders, as well as related molecular genetics, pathophysiology, and epidemiology.
The scope of the Journal covers research into rheumatic diseases where the primary focus relates specifically to a component(s) of the musculoskeletal system.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


