Xuan Nguyen Thanh, Tuan Ngoc Tran, Thuan Nguyen Van, Nguyen Nguyen Duc, Thao Pham Ngoc, Hanh Nguyen Thi, Hoi Nguyen Van, Luyen Nguyen Van
{"title":"Low-dose oral flecainide provocation test for Brugada syndrome: a case series.","authors":"Xuan Nguyen Thanh, Tuan Ngoc Tran, Thuan Nguyen Van, Nguyen Nguyen Duc, Thao Pham Ngoc, Hanh Nguyen Thi, Hoi Nguyen Van, Luyen Nguyen Van","doi":"10.1186/s43044-025-00679-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Brugada syndrome is a rare, inherited cardiac disorder that predisposes individuals to life-threatening ventricular arrhythmias, often leading to sudden cardiac arrest. In many cases, the characteristic electrocardiographic (ECG) findings of Brugada syndrome are not present at baseline but can be unmasked using sodium channel blockers. While intravenous ajmaline is the preferred agent, its limited availability has led to the increased use of oral flecainide for provocation testing. Previous studies have used 300-400 mg doses, but the efficacy and safety of a lower dose, such as 200 mg, have not been systematically evaluated. This report presents three cases demonstrating that a 200 mg oral flecainide dose may be sufficient to unmask the diagnostic Type 1 Brugada ECG pattern in selected patients.</p><p><strong>Case presentation: </strong>Three male patients (aged 44, 48, and 60 years) with suspected Brugada syndrome based on Type 2 ECG patterns underwent flecainide challenge testing. One patient received a 400 mg oral dose, while the other two received 200 mg doses. ECG changes were monitored continuously for 24 h. All three patients developed coved-type ST-segment elevation in the right precordial leads (Type 1 Brugada ECG pattern), confirming the diagnosis. The time to onset of diagnostic ECG changes ranged from 15 to 60 min, with peak changes occurring between 90 min and 5 h. No patients experienced syncope, ventricular arrhythmias, or conduction disturbances during or after testing.</p><p><strong>Conclusions: </strong>This case series suggests that a 200 mg oral flecainide challenge can effectively and safely unmask the diagnostic Type 1 Brugada ECG pattern in selected patients. However, given the small sample size and absence of serum drug concentration data, caution is warranted in interpreting these findings. A lower dose may be a practical alternative to the conventional 400 mg, maintaining diagnostic sensitivity while potentially reducing adverse event risk. Further prospective studies with larger cohorts and longer follow-up are essential to validate the diagnostic performance, safety, and clinical implications of low-dose oral flecainide provocation testing.</p>","PeriodicalId":74993,"journal":{"name":"The Egyptian heart journal : (EHJ) : official bulletin of the Egyptian Society of Cardiology","volume":"77 1","pages":"91"},"PeriodicalIF":0.0000,"publicationDate":"2025-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12504174/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Egyptian heart journal : (EHJ) : official bulletin of the Egyptian Society of Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s43044-025-00679-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Brugada syndrome is a rare, inherited cardiac disorder that predisposes individuals to life-threatening ventricular arrhythmias, often leading to sudden cardiac arrest. In many cases, the characteristic electrocardiographic (ECG) findings of Brugada syndrome are not present at baseline but can be unmasked using sodium channel blockers. While intravenous ajmaline is the preferred agent, its limited availability has led to the increased use of oral flecainide for provocation testing. Previous studies have used 300-400 mg doses, but the efficacy and safety of a lower dose, such as 200 mg, have not been systematically evaluated. This report presents three cases demonstrating that a 200 mg oral flecainide dose may be sufficient to unmask the diagnostic Type 1 Brugada ECG pattern in selected patients.
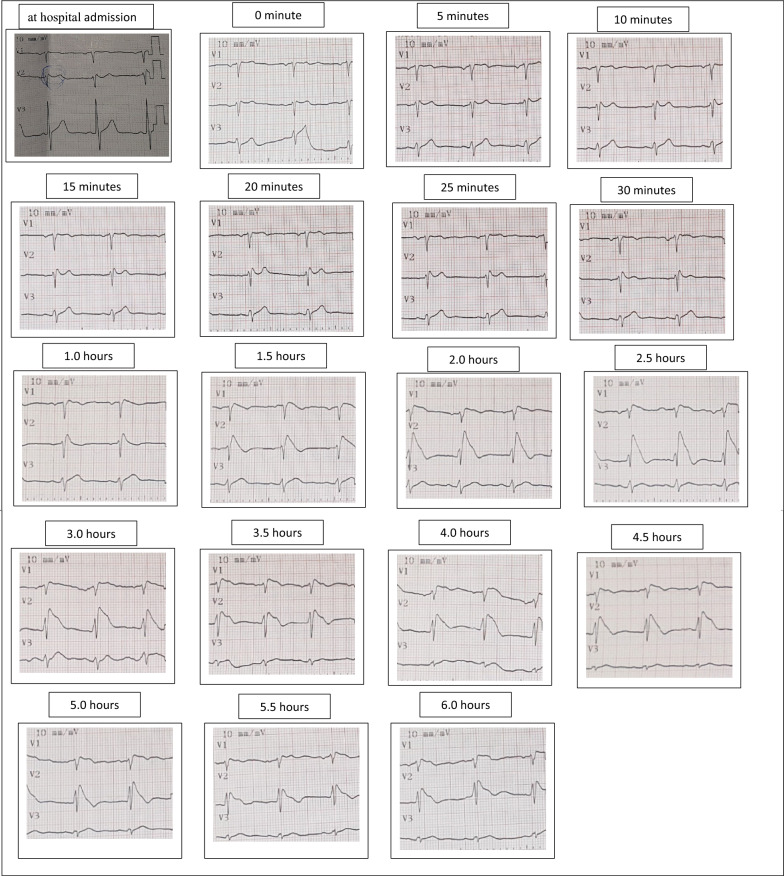
Case presentation: Three male patients (aged 44, 48, and 60 years) with suspected Brugada syndrome based on Type 2 ECG patterns underwent flecainide challenge testing. One patient received a 400 mg oral dose, while the other two received 200 mg doses. ECG changes were monitored continuously for 24 h. All three patients developed coved-type ST-segment elevation in the right precordial leads (Type 1 Brugada ECG pattern), confirming the diagnosis. The time to onset of diagnostic ECG changes ranged from 15 to 60 min, with peak changes occurring between 90 min and 5 h. No patients experienced syncope, ventricular arrhythmias, or conduction disturbances during or after testing.
Conclusions: This case series suggests that a 200 mg oral flecainide challenge can effectively and safely unmask the diagnostic Type 1 Brugada ECG pattern in selected patients. However, given the small sample size and absence of serum drug concentration data, caution is warranted in interpreting these findings. A lower dose may be a practical alternative to the conventional 400 mg, maintaining diagnostic sensitivity while potentially reducing adverse event risk. Further prospective studies with larger cohorts and longer follow-up are essential to validate the diagnostic performance, safety, and clinical implications of low-dose oral flecainide provocation testing.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


