Association of the systemic immune inflammation index with failure after core decompression for osteonecrosis of the femoral head: a prospective time-to-event analysis.
{"title":"Association of the systemic immune inflammation index with failure after core decompression for osteonecrosis of the femoral head: a prospective time-to-event analysis.","authors":"Chengsi Li, Haichuan Guo, Ziyu Han, Tianyu Wang, Dongwei Wu, Zhenbang Yang, Xinqun Cheng, Yingze Zhang, Yanbin Zhu","doi":"10.1080/07853890.2025.2566867","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study aimed to assess the association between preoperative systemic immune inflammation index (SII) and failure after core decompression (CD).</p><p><strong>Methods: </strong>We conducted a prospective study of patients admitted to a tertiary referral hospital with osteonecrosis of the femoral head who underwent CD between October 1, 2014 and April 30, 2019, and provided a minimum 3-year follow-up assessment. Restricted cubic splines assessed the dose-effect relationship between SII and failure. Propensity score matching (PSM) balanced potential preoperative confounders. Kaplan-Meier analyses estimated cumulative incidence as a function of time for the failure between low SII and high SII groups. Multivariable Cox proportional hazards models evaluated the independent association of high SII with failure after adjustment for perioperative factors. Prespecified subgroup analyses explored heterogeneity.</p><p><strong>Results: </strong>We found a positive relationship between the preoperative SII and failure after CD. Among 963 CD procedures performed in 676 patients, failure was observed in 97 cases in a median period of 5.4 years. The cumulative incidence of failure was 10.6% (95% CI, 8.7%, 12.8%) at 5 years. After PSM, failure rates at 5 years were identified as significant differences between the high SII and low SII groups (Log-rank p = 0.019), and that high SII was independently associated with a 1.90-fold (95% CI, 1.14, 3.18; p = 0.014) increased risk of failure. Significant heterogeneity was observed by gender and aetiology (P for interaction < 0.05).</p><p><strong>Conclusions: </strong>Preoperative high SII is a significant risk factor for failure after CD, which could be considered when evaluating surgical indications and providing preoperative counseling to patients.</p>","PeriodicalId":93874,"journal":{"name":"Annals of medicine","volume":"57 1","pages":"2566867"},"PeriodicalIF":4.3000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12502117/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/07853890.2025.2566867","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/10/6 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This study aimed to assess the association between preoperative systemic immune inflammation index (SII) and failure after core decompression (CD).
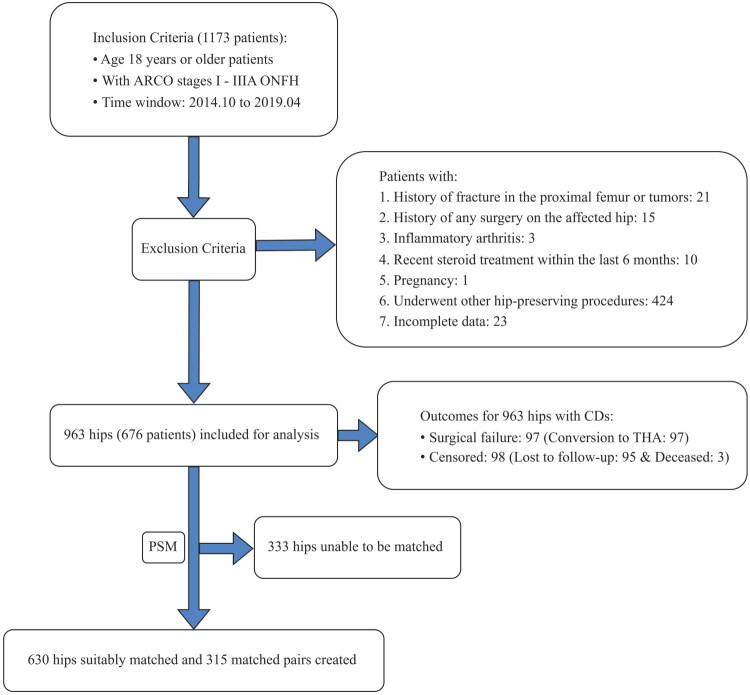
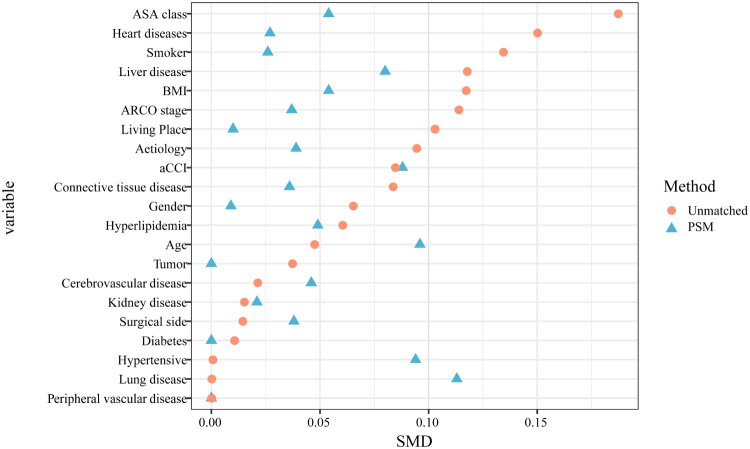
Methods: We conducted a prospective study of patients admitted to a tertiary referral hospital with osteonecrosis of the femoral head who underwent CD between October 1, 2014 and April 30, 2019, and provided a minimum 3-year follow-up assessment. Restricted cubic splines assessed the dose-effect relationship between SII and failure. Propensity score matching (PSM) balanced potential preoperative confounders. Kaplan-Meier analyses estimated cumulative incidence as a function of time for the failure between low SII and high SII groups. Multivariable Cox proportional hazards models evaluated the independent association of high SII with failure after adjustment for perioperative factors. Prespecified subgroup analyses explored heterogeneity.
Results: We found a positive relationship between the preoperative SII and failure after CD. Among 963 CD procedures performed in 676 patients, failure was observed in 97 cases in a median period of 5.4 years. The cumulative incidence of failure was 10.6% (95% CI, 8.7%, 12.8%) at 5 years. After PSM, failure rates at 5 years were identified as significant differences between the high SII and low SII groups (Log-rank p = 0.019), and that high SII was independently associated with a 1.90-fold (95% CI, 1.14, 3.18; p = 0.014) increased risk of failure. Significant heterogeneity was observed by gender and aetiology (P for interaction < 0.05).
Conclusions: Preoperative high SII is a significant risk factor for failure after CD, which could be considered when evaluating surgical indications and providing preoperative counseling to patients.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


