{"title":"Lung ultrasound assessment of pulmonary effects of large patent ductus arteriosus in extremely preterm infants beyond the transitional period.","authors":"Thanaa Elhanafy, Nehad Nasef, Jenna Ibrahim, Rana Awadalla, Amish Jain, Adel Mohamed","doi":"10.1186/s13089-025-00450-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Several studies have suggested a positive association between elevated lung ultrasound scores (LUS) and large patent ductus arteriosus (L-PDA), although findings remain inconsistent. Lung ultrasound score, a semi-quantitative measure of pulmonary aeration loss, has been proposed as a surrogate marker of excessive lung fluid, which may reflect the hemodynamic burden of a significant PDA. The aim of this study was to assess the association between LUS and L-PDA in preterm neonates beyond the initial transitional period and examine its correlations with echocardiographic measures of ductal shunting. This is a cohort retrospective study that included preterm infants born at < 29 weeks' gestation who underwent LUS within 24 h of targeted neonatal echocardiography. Infants were categorized as having L-PDA (diameter ≥ 1.5 mm, left-to-right shunt) or no/small PDA (< 1.5 mm). Clinical characteristics, LUS, and echocardiographic parameters including PDA diameter, left atrial-to-aortic root (LA: Ao) ratio, and left ventricular output (LVO) were compared. Statistical analyses included univariate, multivariate, and correlation assessments.</p><p><strong>Results: </strong>Among 119 infants included in the analysis, 56 (47%) had L-PDA, and 63 (53%) had no or small PDA. Infants with L-PDA had significantly lower gestational age and higher rates of invasive ventilation.</p><p><strong>Lus, la: </strong>Ao ratio, and LVO were significantly elevated in the L-PDA group (all p < 0.001). LUS correlated with PDA diameter (r = 0.27, p = 0.003) and respiratory severity score (r = 0.49, p < 0.001). Furthermore, LUS was found to be independently predictive for L-PDA (adjusted OR 1.5; 95% CI: 1.1-1.9). Each 1-point increase in LUS was associated with a 0.14 mm increase in PDA diameter. Inter-rater reliability for LUS was strong (IRR = 0.86).</p><p><strong>Conclusion: </strong>Beyond the transitional period, LUS was significantly associated with PDA size and independently predicted L-PDA in extremely preterm infants.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":"17 1","pages":"47"},"PeriodicalIF":2.9000,"publicationDate":"2025-10-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12500488/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-025-00450-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Several studies have suggested a positive association between elevated lung ultrasound scores (LUS) and large patent ductus arteriosus (L-PDA), although findings remain inconsistent. Lung ultrasound score, a semi-quantitative measure of pulmonary aeration loss, has been proposed as a surrogate marker of excessive lung fluid, which may reflect the hemodynamic burden of a significant PDA. The aim of this study was to assess the association between LUS and L-PDA in preterm neonates beyond the initial transitional period and examine its correlations with echocardiographic measures of ductal shunting. This is a cohort retrospective study that included preterm infants born at < 29 weeks' gestation who underwent LUS within 24 h of targeted neonatal echocardiography. Infants were categorized as having L-PDA (diameter ≥ 1.5 mm, left-to-right shunt) or no/small PDA (< 1.5 mm). Clinical characteristics, LUS, and echocardiographic parameters including PDA diameter, left atrial-to-aortic root (LA: Ao) ratio, and left ventricular output (LVO) were compared. Statistical analyses included univariate, multivariate, and correlation assessments.
Results: Among 119 infants included in the analysis, 56 (47%) had L-PDA, and 63 (53%) had no or small PDA. Infants with L-PDA had significantly lower gestational age and higher rates of invasive ventilation.
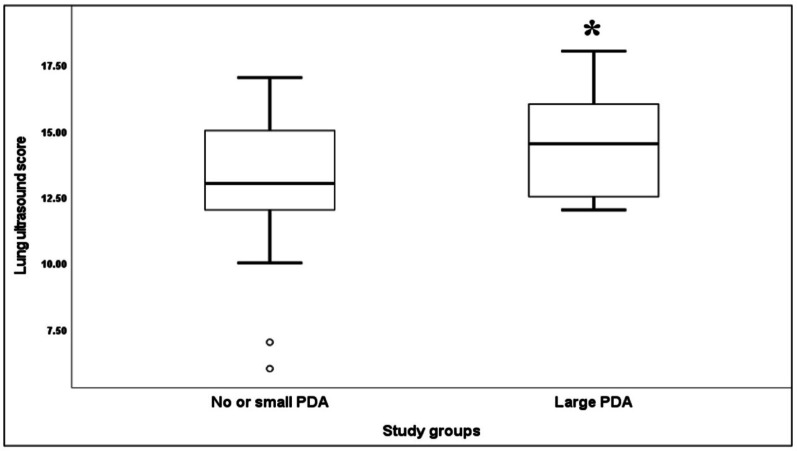
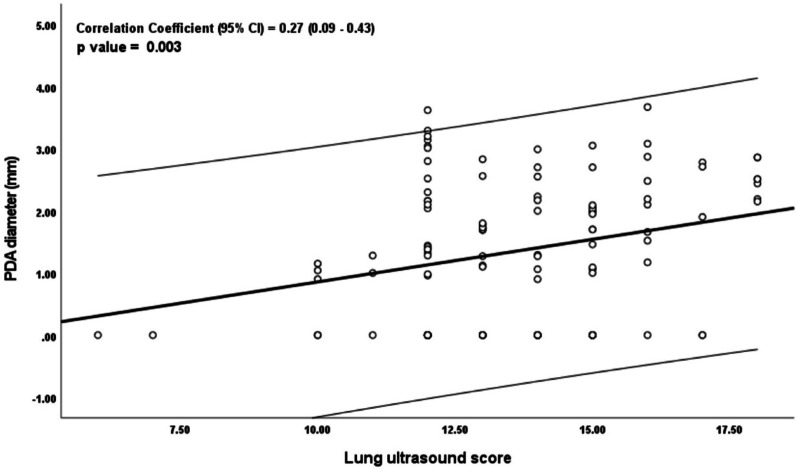
Lus, la: Ao ratio, and LVO were significantly elevated in the L-PDA group (all p < 0.001). LUS correlated with PDA diameter (r = 0.27, p = 0.003) and respiratory severity score (r = 0.49, p < 0.001). Furthermore, LUS was found to be independently predictive for L-PDA (adjusted OR 1.5; 95% CI: 1.1-1.9). Each 1-point increase in LUS was associated with a 0.14 mm increase in PDA diameter. Inter-rater reliability for LUS was strong (IRR = 0.86).
Conclusion: Beyond the transitional period, LUS was significantly associated with PDA size and independently predicted L-PDA in extremely preterm infants.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


