Association and predictability of major perioperative cardiovascular adverse events and elevated neutrophil percentage-to-albumin ratio in patients with stable coronary artery disease undergoing non-cardiac surgery.
{"title":"Association and predictability of major perioperative cardiovascular adverse events and elevated neutrophil percentage-to-albumin ratio in patients with stable coronary artery disease undergoing non-cardiac surgery.","authors":"Haodong Jiang, Jia Zhu, Congying Wang, Xiaojun Xia, Runzhe Wu, Feiyu Chen, Yongquan Niu, Yunpeng Jin","doi":"10.3389/fcvm.2025.1623731","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To evaluate the utility of the preoperative neutrophil percentage-to-albumin ratio (<i>N</i>PAR) for predicting perioperative major adverse cardiovascular events (MACE) in patients with stable coronary artery disease (SCAD) undergoing non-cardiac surgery.</p><p><strong>Methods: </strong>In this retrospective cohort study, we included all adult SCAD patients who underwent non-cardiac surgery at the Fourth Affiliated Hospital of Zhejiang University School of Medicine between October 2020 and October 2024. The primary endpoint was the occurrence of MACE during the perioperative period, defined as a composite of all-cause mortality, cardiac arrest, myocardial infarction, heart failure, or stroke occurring intraoperatively or during the postoperative hospital stay. We used multivariable logistic regression to assess the independent association between NPAR and MACE risk. To explore potential nonlinearity, we fitted smooth curves and performed threshold-effect analysis. Mediation analysis quantified the proportion of the NPAR-MACE relationship explained by estimated glomerular filtration rate (eGFR). Incremental predictive value was evaluated by comparing the area under the receiver operating characteristic curve (AUC), net reclassification improvement (NRI), and integrated discrimination improvement (IDI) before and after adding NPAR to established risk models. Feature selection was conducted using the Boruta algorithm, and predictive performance was further validated with an XGBoost model interpreted via Shapley Additive Explanations (SHAP).</p><p><strong>Results: </strong>Of 1,771 patients, 90 (5.1%) experienced MACE. The MACE subgroup had a higher mean NPAR than those without events (19.4 ± 5.3 vs. 15.9 ± 3.5; <i>P</i> < 0.001). Each 1-unit increase in NPAR was associated with a 20% higher risk of MACE (OR 1.20; 95% CI 1.10-1.30). A J-shaped relationship emerged, with an inflection point at NPAR 13.7 (P_threshold = 0.005). eGFR mediated 8.4% of the NPAR-MACE association. NPAR alone yielded an AUC of 0.721. Adding NPAR to the Revised Cardiac Risk Index raised the AUC from 0.679-0.755 (NRI 0.599; IDI 0.035; all <i>P</i> < 0.01). The XGBoost model achieved an AUC of 0.773, and SHAP analysis identified NPAR as the most influential predictor.</p><p><strong>Conclusions: </strong>Preoperative NPAR is an independent, readily available predictor of perioperative MACE in SCAD patients. Incorporation of NPAR into existing risk models significantly enhances predictive accuracy and may inform targeted perioperative management strategies.</p><p><strong>Results: </strong>Of 1,771 patients, 90 (5.1%) experienced MACE. The MACE subgroup had a higher mean NPAR than those without events (19.4 ± 5.3 vs. 15.9 ± 3.5; <i>P</i> < 0.001). Each 1-unit increase in NPAR was associated with a 20% higher risk of MACE (OR 1.20; 95% CI 1.10-1.30). A J-shaped relationship emerged, with an inflection point at NPAR 13.7 (P_threshold = 0.005). eGFR mediated 8.4% of the NPAR-MACE association. NPAR alone yielded an AUC of 0.721. Adding NPAR to the Revised Cardiac Risk Index raised the AUC from 0.679-0.755 (NRI 0.599; IDI 0.035; all <i>P</i> < 0.01). The XGBoost model achieved an AUC of 0.773, and SHAP analysis identified NPAR as the most influential predictor.</p><p><strong>Conclusions: </strong>Preoperative NPAR is an independent, readily available predictor of perioperative MACE in SCAD patients. Incorporation of NPAR into existing risk models significantly enhances predictive accuracy and may inform targeted perioperative management strategies.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"12 ","pages":"1623731"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12491289/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2025.1623731","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To evaluate the utility of the preoperative neutrophil percentage-to-albumin ratio (NPAR) for predicting perioperative major adverse cardiovascular events (MACE) in patients with stable coronary artery disease (SCAD) undergoing non-cardiac surgery.
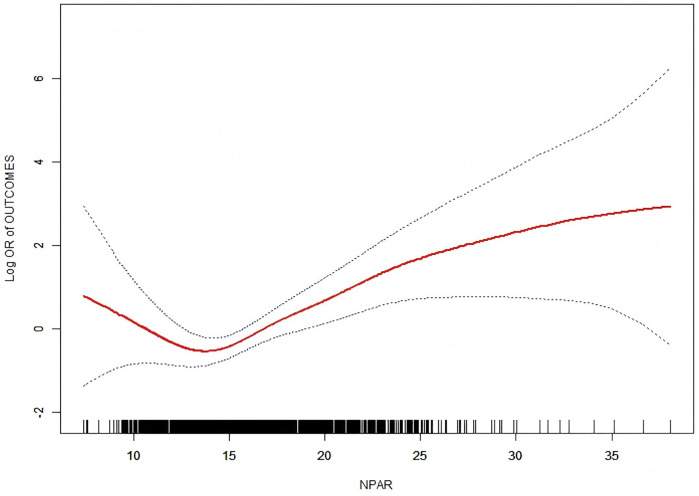
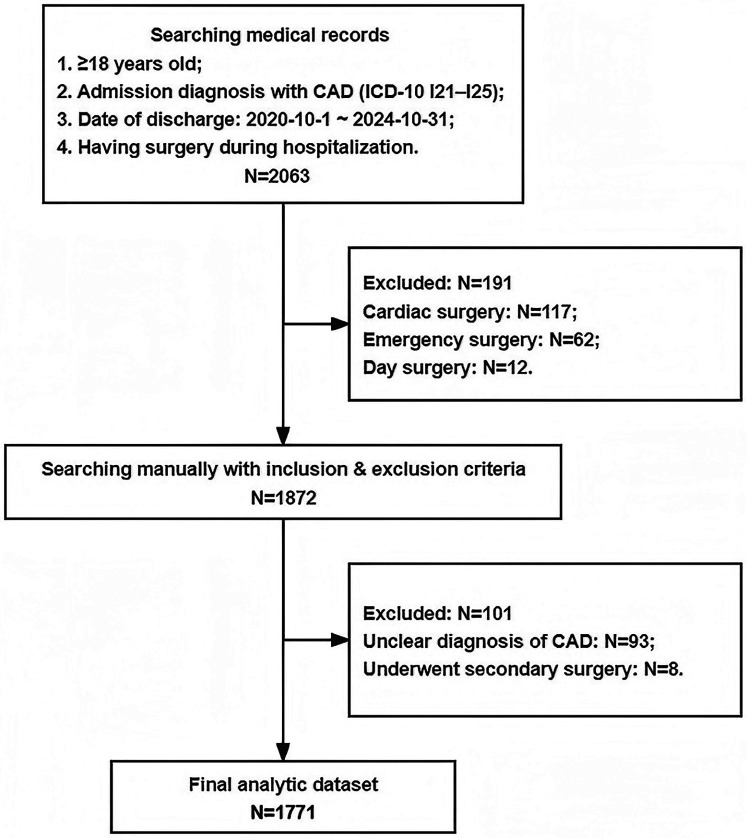
Methods: In this retrospective cohort study, we included all adult SCAD patients who underwent non-cardiac surgery at the Fourth Affiliated Hospital of Zhejiang University School of Medicine between October 2020 and October 2024. The primary endpoint was the occurrence of MACE during the perioperative period, defined as a composite of all-cause mortality, cardiac arrest, myocardial infarction, heart failure, or stroke occurring intraoperatively or during the postoperative hospital stay. We used multivariable logistic regression to assess the independent association between NPAR and MACE risk. To explore potential nonlinearity, we fitted smooth curves and performed threshold-effect analysis. Mediation analysis quantified the proportion of the NPAR-MACE relationship explained by estimated glomerular filtration rate (eGFR). Incremental predictive value was evaluated by comparing the area under the receiver operating characteristic curve (AUC), net reclassification improvement (NRI), and integrated discrimination improvement (IDI) before and after adding NPAR to established risk models. Feature selection was conducted using the Boruta algorithm, and predictive performance was further validated with an XGBoost model interpreted via Shapley Additive Explanations (SHAP).
Results: Of 1,771 patients, 90 (5.1%) experienced MACE. The MACE subgroup had a higher mean NPAR than those without events (19.4 ± 5.3 vs. 15.9 ± 3.5; P < 0.001). Each 1-unit increase in NPAR was associated with a 20% higher risk of MACE (OR 1.20; 95% CI 1.10-1.30). A J-shaped relationship emerged, with an inflection point at NPAR 13.7 (P_threshold = 0.005). eGFR mediated 8.4% of the NPAR-MACE association. NPAR alone yielded an AUC of 0.721. Adding NPAR to the Revised Cardiac Risk Index raised the AUC from 0.679-0.755 (NRI 0.599; IDI 0.035; all P < 0.01). The XGBoost model achieved an AUC of 0.773, and SHAP analysis identified NPAR as the most influential predictor.
Conclusions: Preoperative NPAR is an independent, readily available predictor of perioperative MACE in SCAD patients. Incorporation of NPAR into existing risk models significantly enhances predictive accuracy and may inform targeted perioperative management strategies.
Results: Of 1,771 patients, 90 (5.1%) experienced MACE. The MACE subgroup had a higher mean NPAR than those without events (19.4 ± 5.3 vs. 15.9 ± 3.5; P < 0.001). Each 1-unit increase in NPAR was associated with a 20% higher risk of MACE (OR 1.20; 95% CI 1.10-1.30). A J-shaped relationship emerged, with an inflection point at NPAR 13.7 (P_threshold = 0.005). eGFR mediated 8.4% of the NPAR-MACE association. NPAR alone yielded an AUC of 0.721. Adding NPAR to the Revised Cardiac Risk Index raised the AUC from 0.679-0.755 (NRI 0.599; IDI 0.035; all P < 0.01). The XGBoost model achieved an AUC of 0.773, and SHAP analysis identified NPAR as the most influential predictor.
Conclusions: Preoperative NPAR is an independent, readily available predictor of perioperative MACE in SCAD patients. Incorporation of NPAR into existing risk models significantly enhances predictive accuracy and may inform targeted perioperative management strategies.
目的:评价术前中性粒细胞百分比-白蛋白比(NPAR)在非心脏手术的稳定性冠状动脉疾病(SCAD)患者围手术期主要不良心血管事件(MACE)预测中的应用价值。方法:在这项回顾性队列研究中,我们纳入了2020年10月至2024年10月在浙江大学医学院第四附属医院接受非心脏手术的所有成年SCAD患者。主要终点是围手术期MACE的发生,定义为术中或术后住院期间发生的全因死亡率、心脏骤停、心肌梗死、心力衰竭或中风的综合。我们使用多变量逻辑回归来评估NPAR和MACE风险之间的独立关联。为了探索潜在的非线性,我们拟合了光滑曲线并进行了阈值效应分析。中介分析量化了估算肾小球滤过率(eGFR)解释的NPAR-MACE关系的比例。通过比较在已建立的风险模型中加入NPAR前后的受试者工作特征曲线下面积(AUC)、净重分类改善(NRI)和综合判别改善(IDI)来评估增量预测值。使用Boruta算法进行特征选择,并使用Shapley Additive explanation (SHAP)解释的XGBoost模型进一步验证预测性能。结果:1771例患者中,90例(5.1%)发生MACE。MACE亚组的平均NPAR高于无事件组(19.4±5.3 vs. 15.9±3.5)结论:术前NPAR是SCAD患者围手术期MACE的一个独立的、容易获得的预测指标。将NPAR纳入现有风险模型可显著提高预测准确性,并可为有针对性的围手术期管理策略提供信息。结果:1771例患者中,90例(5.1%)发生MACE。MACE亚组的平均NPAR高于无事件组(19.4±5.3 vs. 15.9±3.5)结论:术前NPAR是SCAD患者围手术期MACE的一个独立的、容易获得的预测指标。将NPAR纳入现有风险模型可显著提高预测准确性,并可为有针对性的围手术期管理策略提供信息。
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


