Solmaz Setayeshgar, Kevin E Liang, Valeria Stoynova, Gillian Frosst, Kate Smolina
{"title":"Modelling the climate impact of inhalers and mitigation strategies: a population-based study in British Columbia, Canada (2015-2032).","authors":"Solmaz Setayeshgar, Kevin E Liang, Valeria Stoynova, Gillian Frosst, Kate Smolina","doi":"10.1136/bmjresp-2025-003218","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Canada has one of the highest per capita greenhouse gas (GHG) emissions, with healthcare contributing ~5% of the total. Pressurised metered-dose inhalers (pMDIs) are significant contributors due to their use of hydrofluorocarbon propellants. While propellant-free dry powder inhalers (DPIs) and soft mist inhalers (SMIs) are available, their adoption remains limited. This population-based study evaluates inhaler dispensation trends in British Columbia (BC), Canada, projects future dispensation and emissions over the next decade, and explores mitigation strategies through pMDI substitution.</p><p><strong>Methods: </strong>Historical inhaler dispensation data (2015-2022) from BC were analysed using negative binomial models to assess trends, project future usage and emissions (2023-2032) and evaluate four substitution scenarios replacing pMDIs with low-GHG alternatives or DPIs/SMIs. Emissions were estimated by inhaler type, sex, age and health region, with uncertainties addressed through Monte Carlo simulation for the projected values.</p><p><strong>Results: </strong>An average of 2.1 million inhalers are dispensed annually in BC, with pMDIs comprising 64% of total inhaler use but contributing 98% of the ~30 000 tonnes of GHG emissions. There was regional variation and older populations contributed disproportionately, reflecting burden of disease. From 2015 to 2022 (excluding 2020 and 2021, the COVID-19 years), pMDI dispensations decreased by 1% annually while DPI/SMI dispensations increased by 5%. Projections show that, without intervention, emissions could rise to ~37 000 tonnes by 2032, varying by age group. All substitution scenarios, by replacing pMDIs with DPIs/SMIs, could reduce emissions by up to 42%.</p><p><strong>Conclusion: </strong>High quality, guideline-directed diagnosis and management of respiratory disease is known to improve health and reduce emissions. Building on these benefits, our analysis shows that substituting pMDIs with lower-emission inhalers, when guided by policy and clinical decisions that prioritise patient safety and preference, can significantly reduce healthcare-related GHG emissions.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"12 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-10-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12496060/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2025-003218","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Canada has one of the highest per capita greenhouse gas (GHG) emissions, with healthcare contributing ~5% of the total. Pressurised metered-dose inhalers (pMDIs) are significant contributors due to their use of hydrofluorocarbon propellants. While propellant-free dry powder inhalers (DPIs) and soft mist inhalers (SMIs) are available, their adoption remains limited. This population-based study evaluates inhaler dispensation trends in British Columbia (BC), Canada, projects future dispensation and emissions over the next decade, and explores mitigation strategies through pMDI substitution.
Methods: Historical inhaler dispensation data (2015-2022) from BC were analysed using negative binomial models to assess trends, project future usage and emissions (2023-2032) and evaluate four substitution scenarios replacing pMDIs with low-GHG alternatives or DPIs/SMIs. Emissions were estimated by inhaler type, sex, age and health region, with uncertainties addressed through Monte Carlo simulation for the projected values.
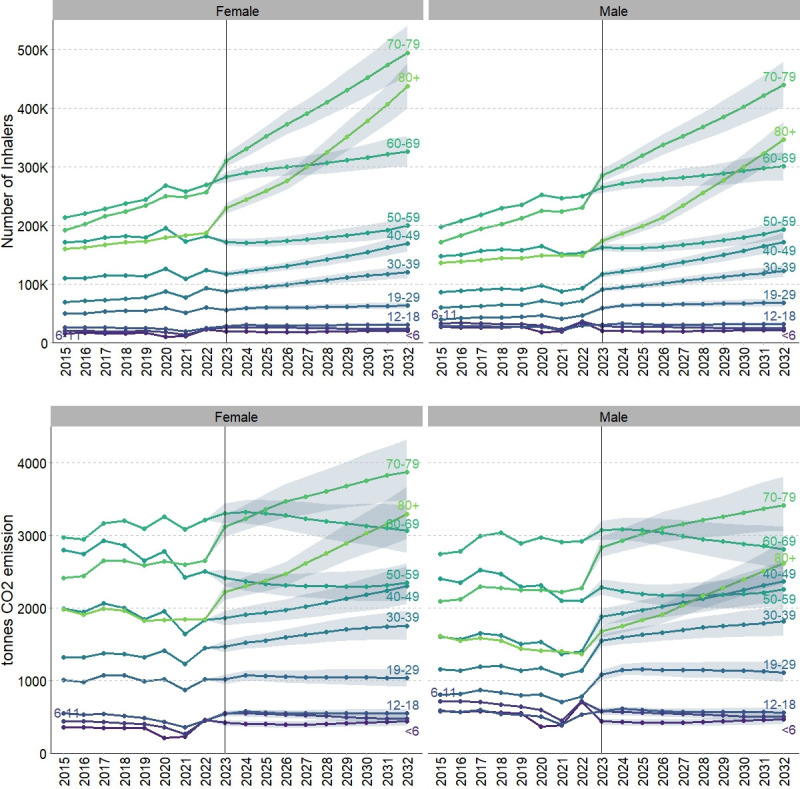
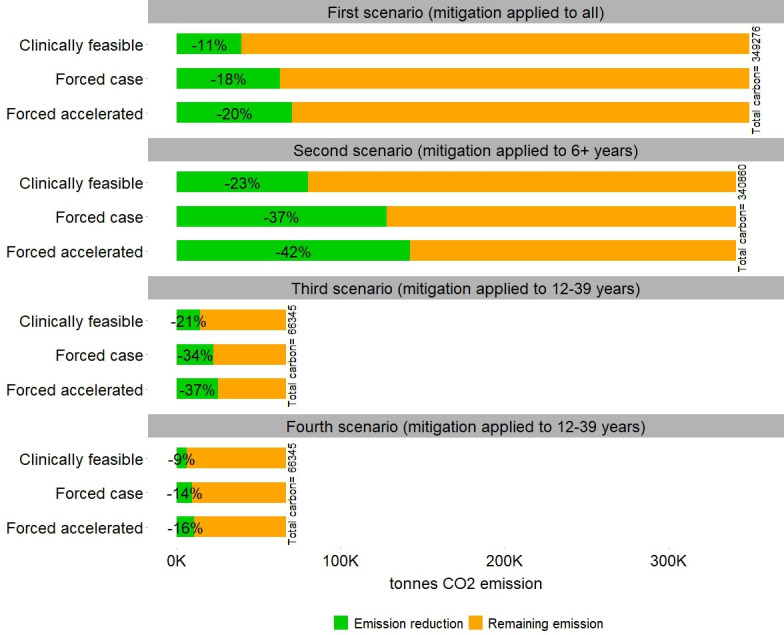
Results: An average of 2.1 million inhalers are dispensed annually in BC, with pMDIs comprising 64% of total inhaler use but contributing 98% of the ~30 000 tonnes of GHG emissions. There was regional variation and older populations contributed disproportionately, reflecting burden of disease. From 2015 to 2022 (excluding 2020 and 2021, the COVID-19 years), pMDI dispensations decreased by 1% annually while DPI/SMI dispensations increased by 5%. Projections show that, without intervention, emissions could rise to ~37 000 tonnes by 2032, varying by age group. All substitution scenarios, by replacing pMDIs with DPIs/SMIs, could reduce emissions by up to 42%.
Conclusion: High quality, guideline-directed diagnosis and management of respiratory disease is known to improve health and reduce emissions. Building on these benefits, our analysis shows that substituting pMDIs with lower-emission inhalers, when guided by policy and clinical decisions that prioritise patient safety and preference, can significantly reduce healthcare-related GHG emissions.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


