{"title":"Longitudinal Cognitive Recovery in Survivors of Critical Illness: Impact of Sepsis and Benzodiazepine Exposure.","authors":"Ruhi Sahu, Ruth-Ann Brown, Anthony S Bonavia","doi":"10.1101/2025.09.23.25336354","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Post-critical illness cognitive dysfunction (PCICD) is a common and debilitating condition affecting survivors of critical illness. While sepsis has been implicated in poor cognitive outcomes, its independent contribution remains unclear due to multiple associated confounders in critical illness. This study aimed to characterize cognitive recovery trajectories over 12 months post-intensive care unit (ICU) and to evaluate the influence of sepsis and benzodiazepine exposure on cognitive outcomes.</p><p><strong>Methods: </strong>In this single-center, prospective cohort study, adult ICU survivors were assessed at 30 days, 3 months, 6 months, and 12 months post-discharge using the telephone-administered Mini-Mental State Examination (MMSE) or Montreal Cognitive Assessment (MoCA). Scores were standardized into <i>z-</i> scores for comparability. Mixed-effects models assessed changes over time and the effects of clinical covariates, including sepsis status and benzodiazepine exposure. Additionally, we investigated whether any one specific cognitive domain was disproportionally impaired by critical illness over time.</p><p><strong>Results: </strong>Of 197 eligible patients during the enrollment period, 77 (39%) completed at least one cognitive assessment. Standardized cognitive scores significantly improved over time, with the greatest gains observed within 6 months: +0.40 SD at 3 months (p = 0.041), +0.54 SD at 6 months (p = 0.016), and +0.49 SD at 12 months (p = 0.033) compared to scores at the time of acute illness. Sepsis status had no significant effect on recovery trajectory. No single cognitive domain was disproportionately affected by critical illness; instead, changes were observed in the overall score over time. Benzodiazepine exposure showed complex associations: longer duration (-0.24 SD/day, p = 0.008) and higher daily dose (-0.02 SD/unit, p = 0.006) were linked to worse cognition, while total cumulative dose was paradoxically associated with better scores (+0.03 SD/unit, p < 0.001), possibly reflecting confounding by indication or survival bias.</p><p><strong>Conclusions: </strong>ICU survivors experience gradual cognitive recovery over the first year, primarily within 6 months. Sepsis does not independently affect this trajectory. Benzodiazepine exposure, especially prolonged or high daily dosing, emerges as a modifiable risk factor for cognitive impairment, consistent with prior investigations of PCICD. These findings highlight the importance of sedation strategies and structured cognitive follow-up.</p>","PeriodicalId":94281,"journal":{"name":"medRxiv : the preprint server for health sciences","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12486035/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"medRxiv : the preprint server for health sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1101/2025.09.23.25336354","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Post-critical illness cognitive dysfunction (PCICD) is a common and debilitating condition affecting survivors of critical illness. While sepsis has been implicated in poor cognitive outcomes, its independent contribution remains unclear due to multiple associated confounders in critical illness. This study aimed to characterize cognitive recovery trajectories over 12 months post-intensive care unit (ICU) and to evaluate the influence of sepsis and benzodiazepine exposure on cognitive outcomes.
Methods: In this single-center, prospective cohort study, adult ICU survivors were assessed at 30 days, 3 months, 6 months, and 12 months post-discharge using the telephone-administered Mini-Mental State Examination (MMSE) or Montreal Cognitive Assessment (MoCA). Scores were standardized into z- scores for comparability. Mixed-effects models assessed changes over time and the effects of clinical covariates, including sepsis status and benzodiazepine exposure. Additionally, we investigated whether any one specific cognitive domain was disproportionally impaired by critical illness over time.
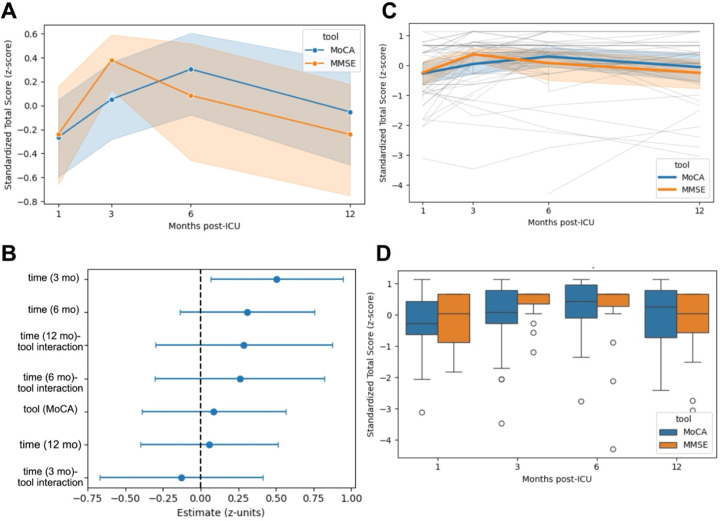
Results: Of 197 eligible patients during the enrollment period, 77 (39%) completed at least one cognitive assessment. Standardized cognitive scores significantly improved over time, with the greatest gains observed within 6 months: +0.40 SD at 3 months (p = 0.041), +0.54 SD at 6 months (p = 0.016), and +0.49 SD at 12 months (p = 0.033) compared to scores at the time of acute illness. Sepsis status had no significant effect on recovery trajectory. No single cognitive domain was disproportionately affected by critical illness; instead, changes were observed in the overall score over time. Benzodiazepine exposure showed complex associations: longer duration (-0.24 SD/day, p = 0.008) and higher daily dose (-0.02 SD/unit, p = 0.006) were linked to worse cognition, while total cumulative dose was paradoxically associated with better scores (+0.03 SD/unit, p < 0.001), possibly reflecting confounding by indication or survival bias.
Conclusions: ICU survivors experience gradual cognitive recovery over the first year, primarily within 6 months. Sepsis does not independently affect this trajectory. Benzodiazepine exposure, especially prolonged or high daily dosing, emerges as a modifiable risk factor for cognitive impairment, consistent with prior investigations of PCICD. These findings highlight the importance of sedation strategies and structured cognitive follow-up.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


