Srinivas Nalloor, G N Impana, Benaganahalli S Sandeep, V N Ranjitha, M Raghavendran, Anish Behl
{"title":"Recurrent hypokalemia induced by primary aldosteronism due to unilateral adrenal adenoma. A case report.","authors":"Srinivas Nalloor, G N Impana, Benaganahalli S Sandeep, V N Ranjitha, M Raghavendran, Anish Behl","doi":"10.4103/jfmpc.jfmpc_2021_24","DOIUrl":null,"url":null,"abstract":"<p><p>Conn's syndrome or primary aldosteronism (PA) due to aldosterone-producing adrenal adenoma (APA) is the most frequent cause of hypokalemia and secondary hypertension. We are reporting a Primary Aldosteronism(PA) case in an indian male, who presented with recurrent lower limb weakness & was admitted twice for management of his symptoms. On evaluating, laboratory reports revealed that his symptoms are due to refractory severe hypokalemia, metabolic alkalosis, raised serum aldosterone levels, and low plasma renin activity. Transtubular potassium gradient (TTKG) was suggestive of ongoing renal potassium loss. Computed Tomography (CT) angiography of adrenal glands during his first admission showed an 8-mm nodule in the right adrenal gland. CT angiography during his second admission with more severe similar complaints revealed an increase in the size of this nodule. The patient was managed with serum potassium correction and surgical intervention. He underwent laparoscopic right adrenalectomy. Following the surgery, the patient serum potassium normalized and he had a good clinical outcome. We suggest clinicians to consider screening for PA and offer surgical intervention wherever necessary in cases with refractory hypokalemia and secondary hypertension.</p>","PeriodicalId":15856,"journal":{"name":"Journal of Family Medicine and Primary Care","volume":"14 8","pages":"3560-3564"},"PeriodicalIF":1.0000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12488115/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Family Medicine and Primary Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jfmpc.jfmpc_2021_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/24 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
引用次数: 0
Abstract
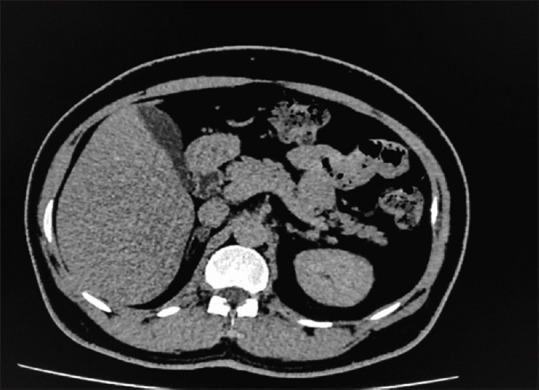
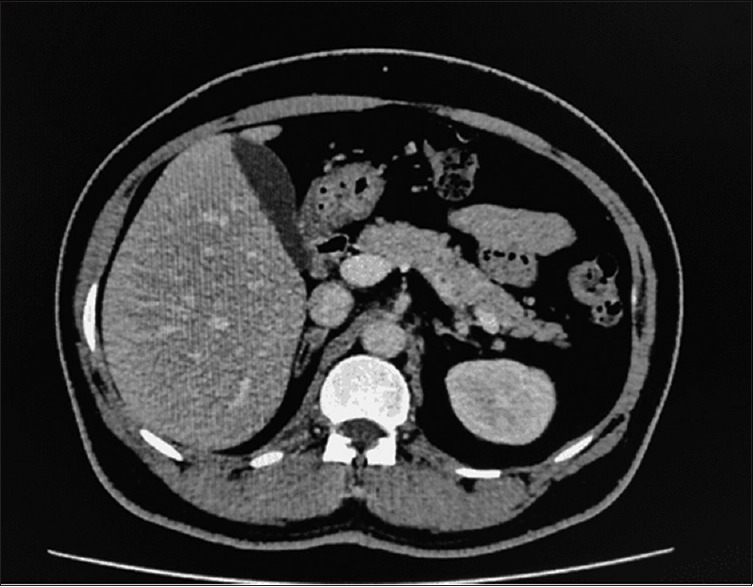
Conn's syndrome or primary aldosteronism (PA) due to aldosterone-producing adrenal adenoma (APA) is the most frequent cause of hypokalemia and secondary hypertension. We are reporting a Primary Aldosteronism(PA) case in an indian male, who presented with recurrent lower limb weakness & was admitted twice for management of his symptoms. On evaluating, laboratory reports revealed that his symptoms are due to refractory severe hypokalemia, metabolic alkalosis, raised serum aldosterone levels, and low plasma renin activity. Transtubular potassium gradient (TTKG) was suggestive of ongoing renal potassium loss. Computed Tomography (CT) angiography of adrenal glands during his first admission showed an 8-mm nodule in the right adrenal gland. CT angiography during his second admission with more severe similar complaints revealed an increase in the size of this nodule. The patient was managed with serum potassium correction and surgical intervention. He underwent laparoscopic right adrenalectomy. Following the surgery, the patient serum potassium normalized and he had a good clinical outcome. We suggest clinicians to consider screening for PA and offer surgical intervention wherever necessary in cases with refractory hypokalemia and secondary hypertension.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


