Complications of microaxial flow pump and VA-ECMO in infarct-related cardiogenic shock: Insights from the Netherlands heart registration
IF 3.2
2区 医学
Q2 CARDIAC & CARDIOVASCULAR SYSTEMS
引用次数: 0
Abstract
Background
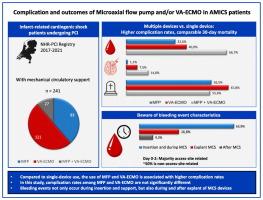
Active mechanical circulatory support (MCS) is associated with high complication rates. Reducing device-related complications may improve outcomes in patients with infarct-related cardiogenic shock (AMI-CS). This study aims to provide in-depth insight in the occurrence, specification and timing of complications in patients receiving active MCS, providing valuable starting points for clinical practice and future studies to reduce complications.
Methods
This real-world, multicentre study, using data from the Netherlands Heart Registration PCI-Registry, describes AMI-CS patients that underwent PCI and received MCS between 2017 and 2021 across 9 Dutch hospitals.
Results
This registry included 241 patients with a mean age of 59.7 years and predominantly male (78.0 %). Microaxial flow pump (MFP), VA-ECMO and MFP + VA-ECMO were used in 93 (38.6 %), 121 (50.2 %) and 27 (11.2 %) patients. MFP + VA-ECMO was associated with highest complication rates, particularly bleeding events (67 % vs. MFP: 33 % vs. VA-ECMO: 40 %). Differences in bleeding events persisted while accounting for competing risk of death (subdistribution hazard ratio (SHR) MFP + VA-ECMO vs. MFP: 2.33 [1.33–4.07]; SHR MFP + VA-ECMO vs. VA-ECMO: 2.00 [1.19–3.36]). SHR for VA-ECMO vs. MFP was 1.18 [0.74–1.90]). Bleeding events were observed within the first days of support, but also on the day of explant and thereafter. Access-site related bleeding events accounted for 51 % of all bleeding events.
Conclusions
Combined use of MFP and VA-ECMO was associated with higher complication rates, particularly bleeding events, compared to single device use. Complication rates between MFP and VA-ECMO were not significantly different. Importantly, patients are still at risk for bleeding events during and after explant of MCS devices.
微轴流泵和VA-ECMO在梗死相关心源性休克中的并发症:来自荷兰心脏登记的见解。
背景:主动机械循环支持(MCS)与高并发症发生率相关。减少器械相关并发症可能改善梗死相关性心源性休克(AMI-CS)患者的预后。本研究旨在深入了解活动期MCS患者并发症的发生、规范和时间,为临床实践和未来减少并发症的研究提供有价值的起点。方法:这项真实世界的多中心研究使用了荷兰心脏登记PCI- registry的数据,描述了2017年至2021年间在9家荷兰医院接受PCI和MCS的AMI-CS患者。结果:该登记包括241例患者,平均年龄59.7 岁,主要为男性(78.0 %)。微轴流泵(MFP)、VA-ECMO和MFP + 分别用于93例(38.6 %)、121例(50.2 %)和27例(11.2 %)患者。MFP + VA-ECMO与最高的并发症发生率相关,特别是出血事件(67 %,MFP: 33 %,VA-ECMO: 40 %)。在考虑竞争死亡风险时,出血事件的差异仍然存在(亚分布风险比(SHR)) MFP + VA-ECMO与MFP: 2.33 [1.33-4.07];月MFP + VA-ECMO vs VA-ECMO: 2.00(1.19 - -3.36))。VA-ECMO与MFP的SHR为1.18[0.74-1.90])。出血事件在支持的第一天内观察到,但也在外植体当天和之后。通路相关出血事件占所有出血事件的51% %。结论:与单独使用MFP和VA-ECMO相比,联合使用MFP和VA-ECMO的并发症发生率更高,特别是出血事件。MFP与VA-ECMO的并发症发生率无显著差异。重要的是,患者在MCS装置移植期间和之后仍然有出血事件的风险。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

International journal of cardiology
医学-心血管系统
CiteScore
6.80
自引率
5.70%
发文量
758
审稿时长
44 days
期刊介绍:
The International Journal of Cardiology is devoted to cardiology in the broadest sense. Both basic research and clinical papers can be submitted. The journal serves the interest of both practicing clinicians and researchers.
In addition to original papers, we are launching a range of new manuscript types, including Consensus and Position Papers, Systematic Reviews, Meta-analyses, and Short communications. Case reports are no longer acceptable. Controversial techniques, issues on health policy and social medicine are discussed and serve as useful tools for encouraging debate.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


