{"title":"The timing of using IVIG for neonatal ABO hemolytic disease.","authors":"Na Ma, Feihong Zhang, Yong Hu, Bin Xia","doi":"10.1186/s12887-025-06062-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>ABO hemolytic disease of the newborn (ABO HDN) is the most prevalent cause of hemolytic disease of the newborn, often leading to hyperbilirubinemia. In some cases, ABO HDN can progress to significant hyperbilirubinemia. The role of intravenous immunoglobulin (IVIG) in treating ABO HDN remains controversial. Several key questions regarding significant hyperbilirubinemia remain unanswered: What are the risk factors of ABO HDN with significant hyperbilirubinemia? Can IVIG provide benefits for ABO HDN with significant hyperbilirubinemia? Where do we place IVIG in the treatment sequence paradigm of ABO HDN? How do we best stratify ABO HDN with significant hyperbilirubinemia for IVIG therapy?</p><p><strong>Methods: </strong>We conducted a retrospective cohort study include 948 newborns from West China Second University Hospital, divided into two groups according to the use/nonuse of IVIG. The maternal and neonatal baseline clinical data were collected from digital medical record system. The risk factors of the significant hyperbilirubinemia associated with ABO HDN were investigated using univariate and multivariate analysis. The generalized additive mixed model (GAMM) was used to analyze the nonlinear relationship of bilirubin level with different treatment over time.</p><p><strong>Results: </strong>A total of 948 newborns fulfilled the inclusion criteria, with 143 (15.1%) in the IVIG group, and 805 (84.9%) in the non-IVIG group. (1) The multivariate analysis found that gestational age ≥ 37 weeks (OR 4.19; p = 0.019), age at admission range 24-48 h (OR 9.69; p = 0.03) and age at admission >48 h (OR 50.31; p < 0.0001) were affect significant hyperbilirubinemia in neonates. (2) The total serum bilirubin (TSB) descent speed of IVIG group (0.69µmol/L/h, 95%CI, 0.48-0.89µmol/L/h) was higher than non-IVIG group (0.21µmol/L/h, 95%CI, 0.14-0.29µmol/L/h) among the neonates with age at admission ≤ 48 h (p < 0.0001);No adverse effects related to IVIG treatment were recorded in either group.</p><p><strong>Conclusion: </strong>Regular monitoring of TSB levels starting 24 h after birth is an effective strategy to prevent severe hyperbilirubinemia in ABO HDN. For southwest Chinese neonates, IVIG should not be routinely used to treat ABO HDN in those admitted > 48 h after birth.</p>","PeriodicalId":9144,"journal":{"name":"BMC Pediatrics","volume":"25 1","pages":"731"},"PeriodicalIF":2.0000,"publicationDate":"2025-10-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12492713/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Pediatrics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12887-025-06062-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: ABO hemolytic disease of the newborn (ABO HDN) is the most prevalent cause of hemolytic disease of the newborn, often leading to hyperbilirubinemia. In some cases, ABO HDN can progress to significant hyperbilirubinemia. The role of intravenous immunoglobulin (IVIG) in treating ABO HDN remains controversial. Several key questions regarding significant hyperbilirubinemia remain unanswered: What are the risk factors of ABO HDN with significant hyperbilirubinemia? Can IVIG provide benefits for ABO HDN with significant hyperbilirubinemia? Where do we place IVIG in the treatment sequence paradigm of ABO HDN? How do we best stratify ABO HDN with significant hyperbilirubinemia for IVIG therapy?
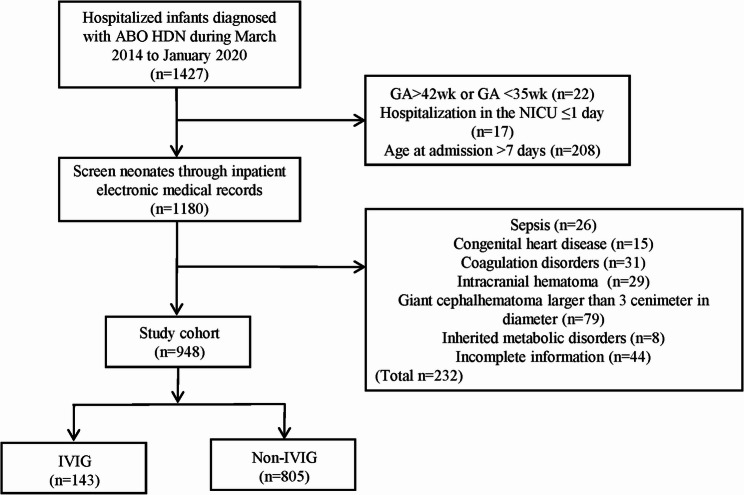
Methods: We conducted a retrospective cohort study include 948 newborns from West China Second University Hospital, divided into two groups according to the use/nonuse of IVIG. The maternal and neonatal baseline clinical data were collected from digital medical record system. The risk factors of the significant hyperbilirubinemia associated with ABO HDN were investigated using univariate and multivariate analysis. The generalized additive mixed model (GAMM) was used to analyze the nonlinear relationship of bilirubin level with different treatment over time.
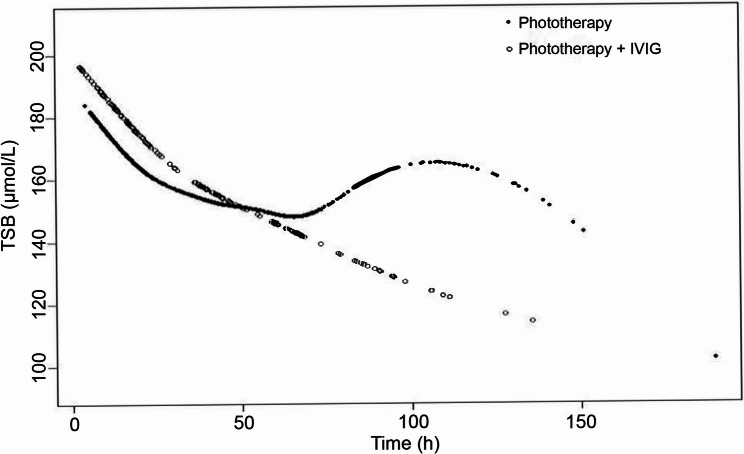
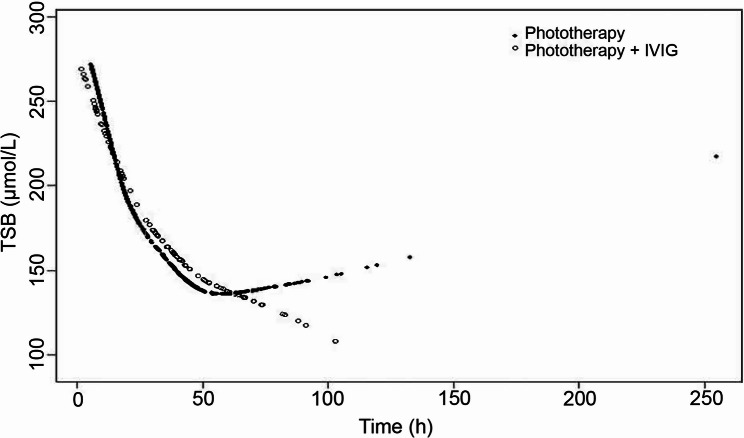
Results: A total of 948 newborns fulfilled the inclusion criteria, with 143 (15.1%) in the IVIG group, and 805 (84.9%) in the non-IVIG group. (1) The multivariate analysis found that gestational age ≥ 37 weeks (OR 4.19; p = 0.019), age at admission range 24-48 h (OR 9.69; p = 0.03) and age at admission >48 h (OR 50.31; p < 0.0001) were affect significant hyperbilirubinemia in neonates. (2) The total serum bilirubin (TSB) descent speed of IVIG group (0.69µmol/L/h, 95%CI, 0.48-0.89µmol/L/h) was higher than non-IVIG group (0.21µmol/L/h, 95%CI, 0.14-0.29µmol/L/h) among the neonates with age at admission ≤ 48 h (p < 0.0001);No adverse effects related to IVIG treatment were recorded in either group.
Conclusion: Regular monitoring of TSB levels starting 24 h after birth is an effective strategy to prevent severe hyperbilirubinemia in ABO HDN. For southwest Chinese neonates, IVIG should not be routinely used to treat ABO HDN in those admitted > 48 h after birth.
期刊介绍:
BMC Pediatrics is an open access journal publishing peer-reviewed research articles in all aspects of health care in neonates, children and adolescents, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


