Comparable Clinical Outcomes with Tiotropium/Olodaterol or Fluticasone Furoate/Umeclidinium/Vilanterol in Patients with COPD and Blood Eosinophil Count ≤300 Cells/μL.
Sanjay Sethi, Brendan Clark, Erin K Buysman, Andrew Sargent, Lindsay G S Bengtson
{"title":"Comparable Clinical Outcomes with Tiotropium/Olodaterol or Fluticasone Furoate/Umeclidinium/Vilanterol in Patients with COPD and Blood Eosinophil Count ≤300 Cells/μL.","authors":"Sanjay Sethi, Brendan Clark, Erin K Buysman, Andrew Sargent, Lindsay G S Bengtson","doi":"10.2147/COPD.S534974","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Assessment of blood eosinophil count (BEC) is recommended to guide the use of inhaled corticosteroids in chronic obstructive pulmonary disease (COPD), with BEC ≥300 cells/μL predictive of patients most likely to benefit.</p><p><strong>Objective: </strong>To compare outcomes between patients initiating dual bronchodilator therapy with tiotropium/olodaterol (TIO/OLO) versus triple therapy with fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI) in patients with COPD and BEC ≤300 cells/μL.</p><p><strong>Methods: </strong>A retrospective cohort study using claims data from the Optum Research Database. Patients with COPD initiated on TIO/OLO or FF/UMEC/VI between 01 June 2015 and 30 November 2019, with a baseline BEC were included. TIO/OLO initiators were 1:1 propensity score matched with FF/UMEC/VI initiators. Time to first exacerbation and pneumonia diagnosis were assessed using Kaplan-Meier analysis. COPD exacerbations and COPD and/or pneumonia-related healthcare resource utilization (HRU) and cost outcomes were presented as population annualized averages.</p><p><strong>Results: </strong>The study population included 3867 individuals with a baseline BEC result. Among these, 3168 (81.9%) had BEC ≤300 cells/μL. After matching, 1098 matched pairs with BEC ≤300 cells/μL were retained. The follow-up annualized count of moderate/severe exacerbations was not significantly different between TIO/OLO and FF/UMEC/VI initiators (1.05 vs 0.99, p=0.535). Annualized counts of COPD and/or pneumonia-related HRU were not significantly different, except for emergency department visits, which were lower for TIO/OLO than FF/UMEC/VI (0.59 vs 0.83, p=0.018). Annualized COPD and/or pneumonia-related emergency department ($370 vs $538, p=0.034) and pharmacy costs ($4692 vs $6573, p<0.001) were lower for TIO/OLO versus FF/UMEC/VI initiators.</p><p><strong>Conclusion: </strong>Eight in ten patients with COPD who initiated FF/UMEC/VI had BEC ≤300 cells/μL. TIO/OLO and FF/UMEC/VI users with BEC ≤300 cells/μL experienced similar rates of COPD exacerbations. TIO/OLO initiators incurred lower pharmacy costs related to COPD and/or pneumonia than FF/UMEC/VI initiators. These results support treatment recommendations of reserving inhaled corticosteroids for frequent exacerbators and patients with elevated eosinophil counts.</p>","PeriodicalId":48818,"journal":{"name":"International Journal of Chronic Obstructive Pulmonary Disease","volume":"20 ","pages":"3327-3338"},"PeriodicalIF":3.1000,"publicationDate":"2025-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12478208/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Chronic Obstructive Pulmonary Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/COPD.S534974","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Assessment of blood eosinophil count (BEC) is recommended to guide the use of inhaled corticosteroids in chronic obstructive pulmonary disease (COPD), with BEC ≥300 cells/μL predictive of patients most likely to benefit.
Objective: To compare outcomes between patients initiating dual bronchodilator therapy with tiotropium/olodaterol (TIO/OLO) versus triple therapy with fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI) in patients with COPD and BEC ≤300 cells/μL.
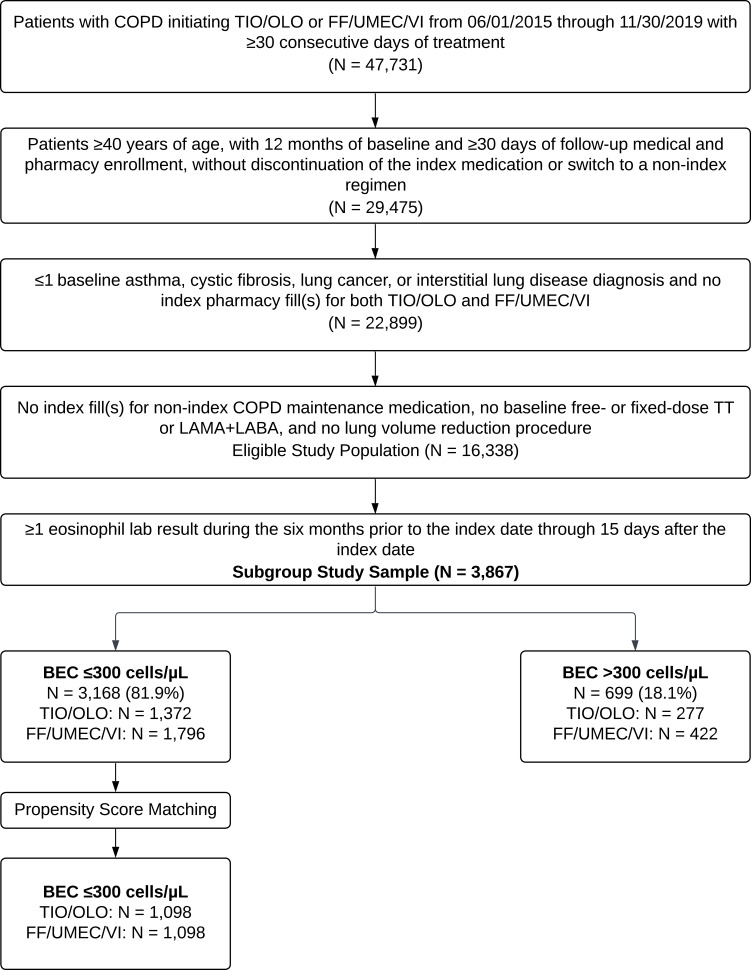
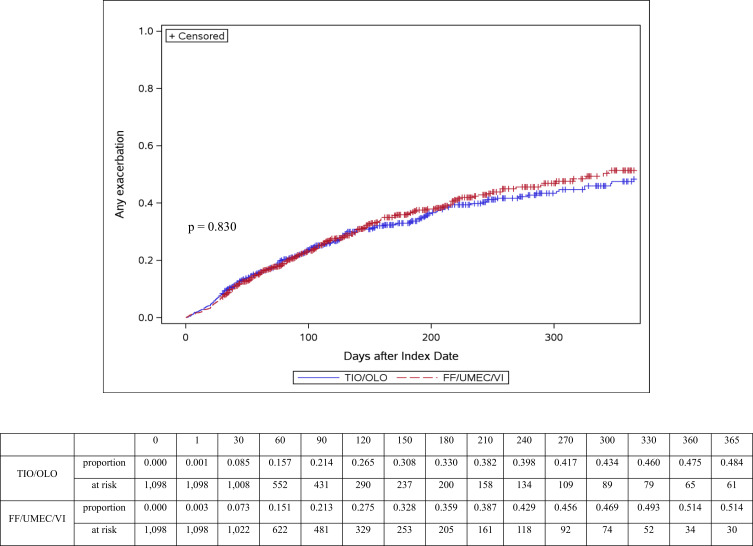
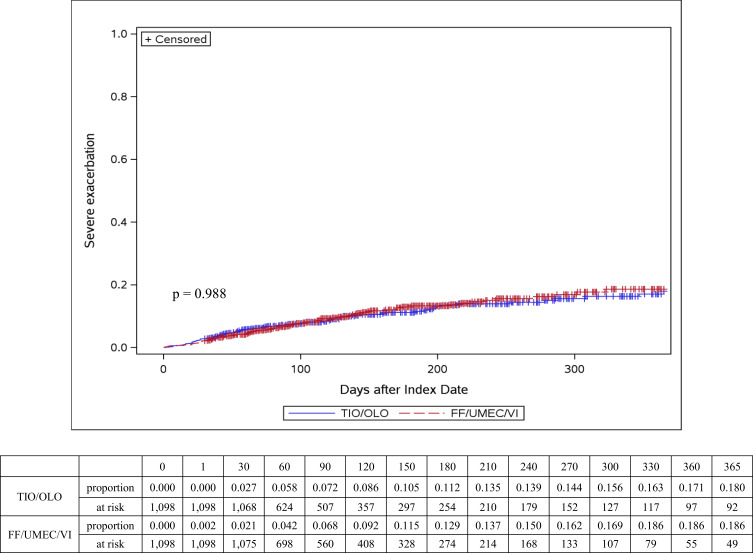
Methods: A retrospective cohort study using claims data from the Optum Research Database. Patients with COPD initiated on TIO/OLO or FF/UMEC/VI between 01 June 2015 and 30 November 2019, with a baseline BEC were included. TIO/OLO initiators were 1:1 propensity score matched with FF/UMEC/VI initiators. Time to first exacerbation and pneumonia diagnosis were assessed using Kaplan-Meier analysis. COPD exacerbations and COPD and/or pneumonia-related healthcare resource utilization (HRU) and cost outcomes were presented as population annualized averages.
Results: The study population included 3867 individuals with a baseline BEC result. Among these, 3168 (81.9%) had BEC ≤300 cells/μL. After matching, 1098 matched pairs with BEC ≤300 cells/μL were retained. The follow-up annualized count of moderate/severe exacerbations was not significantly different between TIO/OLO and FF/UMEC/VI initiators (1.05 vs 0.99, p=0.535). Annualized counts of COPD and/or pneumonia-related HRU were not significantly different, except for emergency department visits, which were lower for TIO/OLO than FF/UMEC/VI (0.59 vs 0.83, p=0.018). Annualized COPD and/or pneumonia-related emergency department ($370 vs $538, p=0.034) and pharmacy costs ($4692 vs $6573, p<0.001) were lower for TIO/OLO versus FF/UMEC/VI initiators.
Conclusion: Eight in ten patients with COPD who initiated FF/UMEC/VI had BEC ≤300 cells/μL. TIO/OLO and FF/UMEC/VI users with BEC ≤300 cells/μL experienced similar rates of COPD exacerbations. TIO/OLO initiators incurred lower pharmacy costs related to COPD and/or pneumonia than FF/UMEC/VI initiators. These results support treatment recommendations of reserving inhaled corticosteroids for frequent exacerbators and patients with elevated eosinophil counts.
期刊介绍:
An international, peer-reviewed journal of therapeutics and pharmacology focusing on concise rapid reporting of clinical studies and reviews in COPD. Special focus will be given to the pathophysiological processes underlying the disease, intervention programs, patient focused education, and self management protocols. This journal is directed at specialists and healthcare professionals

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


