Mayam Roze Ahvazi, Mohammad Adineh, Mohsen Savaie, Saeed Ghanbari
{"title":"Effect of a patient-ventilator asynchrony (PVA) management protocol on treatment outcomes in ICU patients: a randomized controlled trial.","authors":"Mayam Roze Ahvazi, Mohammad Adineh, Mohsen Savaie, Saeed Ghanbari","doi":"10.1186/s13104-025-07467-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Mechanical ventilation is a critical life support for ICU patients. However, this intervention can be associated with complications such as patient-ventilator asynchrony (PVA) and subsequent adverse events. This study aimed to investigate the impact of implementing a PVA management protocol on clinical outcomes in ICU patients.</p><p><strong>Methods: </strong>In this single-blind randomized controlled trial conducted from January to August 2024, a total of 66 mechanically ventilated patients admitted to the ICU of a hospital affiliated with Ahvaz Jundishapur University of Medical Sciences (Ahvaz, Iran) were randomly allocated to either an intervention or control group using a permuted block randomization method. Patients in the intervention group were evaluated for patient-ventilator asynchrony (PVA) every two hours throughout their ICU stay, as long as they remained on mechanical ventilation. If PVA was detected, appropriate interventions were implemented in accordance with the protocol of PVA management. The control group received routine care without a specific PVA management protocol. Data were collected using a structured checklist and analyzed using SPSS version 22. This study registered in the Iranian Registry of Clinical Trials (IRCT20231001059572N1).</p><p><strong>Results: </strong>There was a significant difference between the intervention and control groups in terms of duration of mechanical ventilation (p < 0.001), length of ICU stay (p < 0.001), and successful weaning from the ventilator (p < 0.001). In all three dimensions, the intervention group showed better outcomes. However, there was no significant difference between the two groups in terms of ICU mortality (p = 0.202) and self-extubation (p = 0.787). Being in the intervention group was the strongest predictive factor for length of ICU stay (β = -8.268, p < 0.001) and duration of mechanical ventilation (β = -3.906, p = 0.003). No major harms or unintended adverse effects were reported related to the intervention.</p><p><strong>Conclusion: </strong>Implementation of a PVA management protocol was associated with improved clinical outcomes, including reduced duration of mechanical ventilation, shorter ICU stays, and higher rates of successful weaning. Given its simplicity, cost-effectiveness, and the favorable results observed, broader adoption of this protocol in ICU settings is recommended. Further studies are warranted to confirm these findings and examine their generalizability across different clinical contexts.</p>","PeriodicalId":9234,"journal":{"name":"BMC Research Notes","volume":"18 1","pages":"396"},"PeriodicalIF":1.7000,"publicationDate":"2025-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12487041/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Research Notes","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13104-025-07467-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Mechanical ventilation is a critical life support for ICU patients. However, this intervention can be associated with complications such as patient-ventilator asynchrony (PVA) and subsequent adverse events. This study aimed to investigate the impact of implementing a PVA management protocol on clinical outcomes in ICU patients.
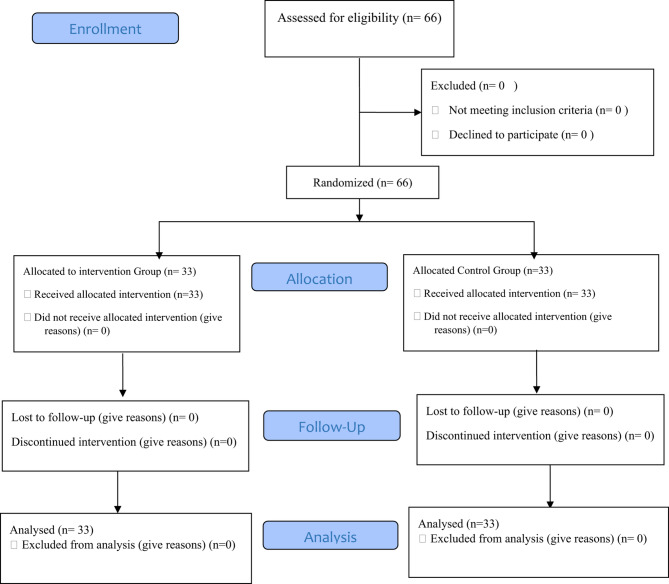
Methods: In this single-blind randomized controlled trial conducted from January to August 2024, a total of 66 mechanically ventilated patients admitted to the ICU of a hospital affiliated with Ahvaz Jundishapur University of Medical Sciences (Ahvaz, Iran) were randomly allocated to either an intervention or control group using a permuted block randomization method. Patients in the intervention group were evaluated for patient-ventilator asynchrony (PVA) every two hours throughout their ICU stay, as long as they remained on mechanical ventilation. If PVA was detected, appropriate interventions were implemented in accordance with the protocol of PVA management. The control group received routine care without a specific PVA management protocol. Data were collected using a structured checklist and analyzed using SPSS version 22. This study registered in the Iranian Registry of Clinical Trials (IRCT20231001059572N1).
Results: There was a significant difference between the intervention and control groups in terms of duration of mechanical ventilation (p < 0.001), length of ICU stay (p < 0.001), and successful weaning from the ventilator (p < 0.001). In all three dimensions, the intervention group showed better outcomes. However, there was no significant difference between the two groups in terms of ICU mortality (p = 0.202) and self-extubation (p = 0.787). Being in the intervention group was the strongest predictive factor for length of ICU stay (β = -8.268, p < 0.001) and duration of mechanical ventilation (β = -3.906, p = 0.003). No major harms or unintended adverse effects were reported related to the intervention.
Conclusion: Implementation of a PVA management protocol was associated with improved clinical outcomes, including reduced duration of mechanical ventilation, shorter ICU stays, and higher rates of successful weaning. Given its simplicity, cost-effectiveness, and the favorable results observed, broader adoption of this protocol in ICU settings is recommended. Further studies are warranted to confirm these findings and examine their generalizability across different clinical contexts.
背景:机械通气是ICU患者重要的生命支持手段。然而,这种干预可能与并发症相关,如患者-呼吸机不同步(PVA)和随后的不良事件。本研究旨在探讨实施PVA管理方案对ICU患者临床结局的影响。方法:本研究于2024年1 - 8月在伊朗阿瓦士Jundishapur医科大学附属医院ICU进行单盲随机对照试验,采用排列块随机法将66例机械通气患者随机分为干预组和对照组。干预组患者在ICU住院期间每两小时对患者-呼吸机不同步(PVA)进行评估,只要他们仍然使用机械通气。如果检测到PVA,则按照PVA管理方案实施适当的干预措施。对照组接受常规护理,无特殊PVA管理方案。使用结构化检查表收集数据,并使用SPSS version 22进行分析。本研究已在伊朗临床试验登记处注册(IRCT20231001059572N1)。结果:干预组与对照组在机械通气持续时间方面存在显著差异(p结论:PVA管理方案的实施与改善临床结果相关,包括机械通气持续时间缩短、ICU住院时间缩短和脱机成功率提高。鉴于其简单、成本效益和观察到的良好结果,建议在ICU环境中更广泛地采用该方案。需要进一步的研究来证实这些发现,并检验它们在不同临床背景下的普遍性。
BMC Research NotesBiochemistry, Genetics and Molecular Biology-Biochemistry, Genetics and Molecular Biology (all)
CiteScore
3.60
自引率
0.00%
发文量
363
审稿时长
15 weeks
期刊介绍:
BMC Research Notes publishes scientifically valid research outputs that cannot be considered as full research or methodology articles. We support the research community across all scientific and clinical disciplines by providing an open access forum for sharing data and useful information; this includes, but is not limited to, updates to previous work, additions to established methods, short publications, null results, research proposals and data management plans.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


