Miri Dotan, Dror Rosengarten, Karam Azem, Shai Fein, Yael Shostak, Dorit Shitenberg, Yuri Peysakhovich, Yaron D Barac, Elizabeth Fireman, Paul Blanc, Osnat Shtraichman, Mordechai Reuven Kramer
{"title":"Single versus double lung transplantation outcomes in artificial stone silicosis: a single-centre retrospective cohort study.","authors":"Miri Dotan, Dror Rosengarten, Karam Azem, Shai Fein, Yael Shostak, Dorit Shitenberg, Yuri Peysakhovich, Yaron D Barac, Elizabeth Fireman, Paul Blanc, Osnat Shtraichman, Mordechai Reuven Kramer","doi":"10.1136/bmjresp-2024-002703","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Silicosis, caused by inhaling crystalline silica, is a growing global health concern exacerbated by the increased use of artificial stone. In end-stage silicosis, lung transplantation may be the only available treatment. While double lung transplantation has long-term survival benefits over single lung transplantation, this issue was not assessed in patients with silicosis.</p><p><strong>Research question: </strong>Our study aimed to evaluate survival outcomes in silicosis patients undergoing lung transplantation, comparing single versus double lung transplants.</p><p><strong>Study design and methods: </strong>This is a single-centre retrospective cohort study of all patients who underwent lung transplantation for silicosis at our centre between March 2006 and March 2024.</p><p><strong>Results: </strong>During the study period, our centre conducted 778 lung transplantations, 40 of them (5.14%) were for silicosis, 25 single lung transplants and 15 double lung transplants. Double lung transplantation recipients experienced a more challenging surgical course due to adhesions and difficulty in explantation, associated with a significantly higher volume of blood products (8.00±15.13 units vs 24.85±24.41 units, p=0.023) and longer ischaemic times (243.63±85.36 min vs 327.67±95.23 min, p=0.009). There was no significant difference in the risk of death or re-transplantation in the single lung versus the double lung group (HR 1.163, 95% CI 0.473 to 2.861; p=0.74). Additionally, the two groups had no significant disparities in pulmonary function test results at 1 and 3 years post-transplant (51.93±22.43 vs 66.67±32.09 forced expiratory volume in the first second percent predicted at 36 months follow-up, p=0.25).</p><p><strong>Conclusion: </strong>Given the intricate surgical procedure required for transplanting lungs in cases of silicosis, longer ischaemic times, increased need for blood products and the absence of definitive evidence supporting double lung transplantation in this population, it may be prudent to contemplate prioritising single lung transplantation for these patients.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"12 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-09-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12481386/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2024-002703","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Silicosis, caused by inhaling crystalline silica, is a growing global health concern exacerbated by the increased use of artificial stone. In end-stage silicosis, lung transplantation may be the only available treatment. While double lung transplantation has long-term survival benefits over single lung transplantation, this issue was not assessed in patients with silicosis.
Research question: Our study aimed to evaluate survival outcomes in silicosis patients undergoing lung transplantation, comparing single versus double lung transplants.
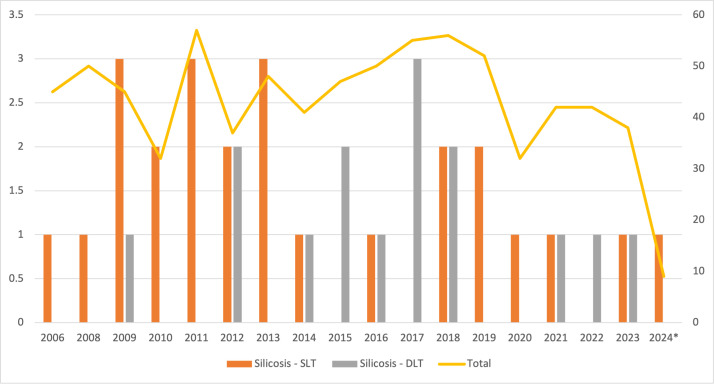
Study design and methods: This is a single-centre retrospective cohort study of all patients who underwent lung transplantation for silicosis at our centre between March 2006 and March 2024.
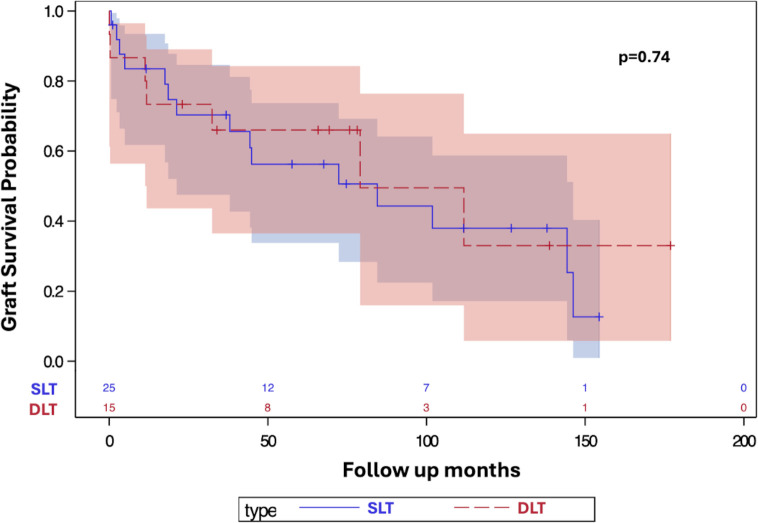
Results: During the study period, our centre conducted 778 lung transplantations, 40 of them (5.14%) were for silicosis, 25 single lung transplants and 15 double lung transplants. Double lung transplantation recipients experienced a more challenging surgical course due to adhesions and difficulty in explantation, associated with a significantly higher volume of blood products (8.00±15.13 units vs 24.85±24.41 units, p=0.023) and longer ischaemic times (243.63±85.36 min vs 327.67±95.23 min, p=0.009). There was no significant difference in the risk of death or re-transplantation in the single lung versus the double lung group (HR 1.163, 95% CI 0.473 to 2.861; p=0.74). Additionally, the two groups had no significant disparities in pulmonary function test results at 1 and 3 years post-transplant (51.93±22.43 vs 66.67±32.09 forced expiratory volume in the first second percent predicted at 36 months follow-up, p=0.25).
Conclusion: Given the intricate surgical procedure required for transplanting lungs in cases of silicosis, longer ischaemic times, increased need for blood products and the absence of definitive evidence supporting double lung transplantation in this population, it may be prudent to contemplate prioritising single lung transplantation for these patients.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


