The role of seasonal malaria chemoprevention in the effect of azithromycin on child mortality: A secondary analysis of the CHAT cluster randomized clinical trial.
Elisabeth A Gebreegziabher, Mamadou Ouattara, Mamadou Bountogo, Boubacar Coulibaly, Valentin Boudo, Thierry Ouedraogo, Elodie Lebas, Huiyu Hu, Kieran S O'Brien, Michelle S Hsiang, David V Glidden, Benjamin F Arnold, Thomas M Lietman, Ali Sié, Catherine E Oldenburg
{"title":"The role of seasonal malaria chemoprevention in the effect of azithromycin on child mortality: A secondary analysis of the CHAT cluster randomized clinical trial.","authors":"Elisabeth A Gebreegziabher, Mamadou Ouattara, Mamadou Bountogo, Boubacar Coulibaly, Valentin Boudo, Thierry Ouedraogo, Elodie Lebas, Huiyu Hu, Kieran S O'Brien, Michelle S Hsiang, David V Glidden, Benjamin F Arnold, Thomas M Lietman, Ali Sié, Catherine E Oldenburg","doi":"10.1371/journal.pgph.0004653","DOIUrl":null,"url":null,"abstract":"<p><p>The objective of this study was to examine whether the effect of mass Azithromycin (AZ) distribution on all-cause mortality among children under 5 varies with seasonal malaria chemoprevention (SMC) administration season or coverage. This was a secondary analysis of the Community Health with Azithromycin Trial (CHAT), a cluster-randomized, placebo-controlled trial of twice-yearly AZ treatment in 341 communities in the Nouna District, Burkina Faso. All communities received SMC as standard-of-care. SMC administration and coverage data were provided from National Malaria Control Program. SMC season was defined as the period during and following SMC (July-December) versus the no SMC season (January-June). SMC coverage was assessed as proportion of the population covered and by whether it was below or above a threshold of 80%. We used Poisson regression models with person-time at risk as an offset and robust standard error to analyze mortality rates by treatment group and SMC subgroups and assessed interaction on both multiplicative and additive scales. Mortality was higher in SMC seasons for both arms. Compared to placebo, the mortality rate in AZ clusters was 0.77 (95% CI: 0.60 to 0.98) during SMC season, while it was 0.89 (95% CI: 0.68 to 1.15) during the non-SMC seasons. In clusters with <80% SMC coverage, the effect of AZ was 0.73 95%CI (0.56 to 0.96) and in clusters with ≥80% SMC coverage, it was 1.0 95%CI (0.59 to 1.69). The interaction between AZ and SMC season or coverage was not statistically significant on the additive or multiplicative scales. While our findings did not reach statistical significance, they raise the question of whether prioritizing MDA AZ during high transmission periods or in regions with low SMC coverage could be beneficial. Further research is needed to determine if targeting these periods or areas could further reduce child mortality.</p>","PeriodicalId":74466,"journal":{"name":"PLOS global public health","volume":"5 9","pages":"e0004653"},"PeriodicalIF":2.5000,"publicationDate":"2025-09-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12478956/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLOS global public health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1371/journal.pgph.0004653","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
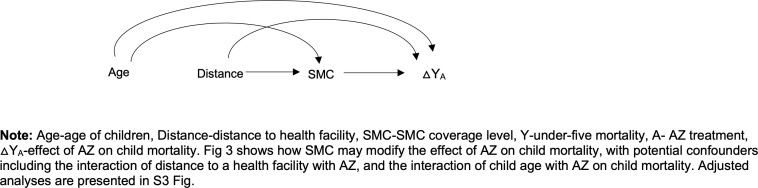
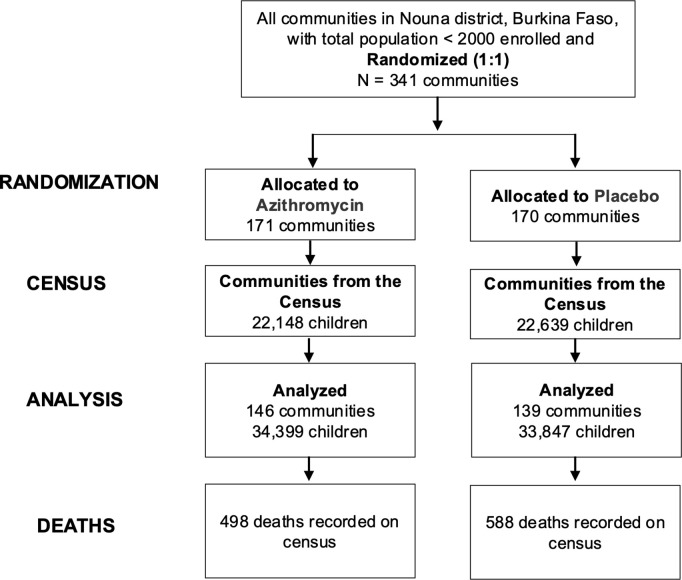
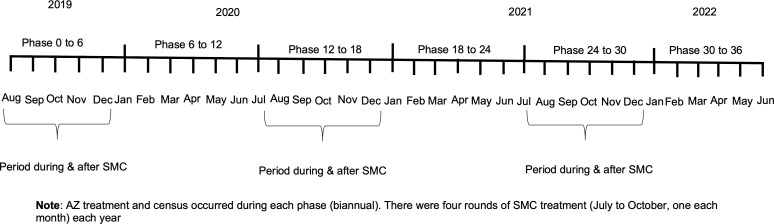
The objective of this study was to examine whether the effect of mass Azithromycin (AZ) distribution on all-cause mortality among children under 5 varies with seasonal malaria chemoprevention (SMC) administration season or coverage. This was a secondary analysis of the Community Health with Azithromycin Trial (CHAT), a cluster-randomized, placebo-controlled trial of twice-yearly AZ treatment in 341 communities in the Nouna District, Burkina Faso. All communities received SMC as standard-of-care. SMC administration and coverage data were provided from National Malaria Control Program. SMC season was defined as the period during and following SMC (July-December) versus the no SMC season (January-June). SMC coverage was assessed as proportion of the population covered and by whether it was below or above a threshold of 80%. We used Poisson regression models with person-time at risk as an offset and robust standard error to analyze mortality rates by treatment group and SMC subgroups and assessed interaction on both multiplicative and additive scales. Mortality was higher in SMC seasons for both arms. Compared to placebo, the mortality rate in AZ clusters was 0.77 (95% CI: 0.60 to 0.98) during SMC season, while it was 0.89 (95% CI: 0.68 to 1.15) during the non-SMC seasons. In clusters with <80% SMC coverage, the effect of AZ was 0.73 95%CI (0.56 to 0.96) and in clusters with ≥80% SMC coverage, it was 1.0 95%CI (0.59 to 1.69). The interaction between AZ and SMC season or coverage was not statistically significant on the additive or multiplicative scales. While our findings did not reach statistical significance, they raise the question of whether prioritizing MDA AZ during high transmission periods or in regions with low SMC coverage could be beneficial. Further research is needed to determine if targeting these periods or areas could further reduce child mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


