{"title":"Tailoring treatment for esophageal cancer: a retrospective comparison of chemoradiation with and without esophagectomy.","authors":"Piyapasara Toapichattrakul, Kittinon Santasup, Kittisak Kittirungsi, Thanapat Seemakajohn, Phubodee Kittiwan, Ausareeya Chumachote, Bandhuphat Chakrabandhu, Somvilai Chakrabandhu","doi":"10.1186/s12893-025-03211-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Locally advanced esophageal cancer remains a significant therapeutic challenge, with the optimal treatment strategy still debate. While previous studies suggest that concurrent chemoradiation therapy (CCRT) can improve survival, the role of esophagectomy following CCRT in patients with partial or no response has not been well-characterized, particularly in resource-limited settings. This study aimed to evaluate the survival benefit of esophagectomy following CCRT, with particular focus on non-complete responders (non-CR).</p><p><strong>Methods: </strong>We conducted a retrospective cohort study of 132 patients with locally advanced esophageal cancer treated at Maharaj Nakorn Chiang Mai Hospital between 2013 and 2022. Patients were categorized based on initial treatment into preoperative CCRT or definitive CCRT groups. Overall survival (OS) and progression-free survival (PFS) were compared using multivariable Cox regression. A secondary analysis stratified patients into three groups by clinical response and surgical status: CR without surgery, non-CR with surgery, and non-CR without surgery. To reduce baseline imbalances and selection bias, inverse probability of treatment weighting (IPTW) was applied in the non-CR subgroup initially intended for preoperative CCRT.</p><p><strong>Results: </strong>Baseline characteristics were balanced except for tumor location. Median follow-up was 1.23 years (IQR: 0.64-2.50). Overall, 1-/2-year PFS was 27.97%/17.80%, while OS was 60.47%/37.33%. Median survival did not differ between preoperative versus definitive CCRT (1.20 vs. 1.52 years, p = 0.346). However, in the surgical-status analysis, patients undergoing post-CCRT esophagectomy showed significantly improved PFS and OS versus non-surgical non-CR patients (PFS HR: 2.89, p < 0.001; OS HR: 2.97, p = 0.001). Notably, surgical non-CR patients achieved OS comparable to CR patients without esophagectomy (HR: 1.12, p = 0.812). To minimize selection bias, we conducted an IPTW-adjusted analysis in the subgroup of non-CR patients initially assigned to preoperative CCRT. After IPTW, the survival benefit of surgery remained significant, with improved PFS (HR: 3.75; 95% CI: 1.40-10.08; p = 0.009) and OS (HR: 2.74; 95% CI: 1.57-4.77; p < 0.001) compared to CCRT alone.</p><p><strong>Conclusion: </strong>Esophagectomy after CCRT provides survival benefits equivalent to achieving CR with CCRT alone, particularly for non-CR patients. These results advocate for surgical integration as a salvage strategy for incomplete responders in locally advanced esophageal cancer.</p>","PeriodicalId":49229,"journal":{"name":"BMC Surgery","volume":"25 1","pages":"417"},"PeriodicalIF":1.8000,"publicationDate":"2025-09-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12482222/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12893-025-03211-1","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Locally advanced esophageal cancer remains a significant therapeutic challenge, with the optimal treatment strategy still debate. While previous studies suggest that concurrent chemoradiation therapy (CCRT) can improve survival, the role of esophagectomy following CCRT in patients with partial or no response has not been well-characterized, particularly in resource-limited settings. This study aimed to evaluate the survival benefit of esophagectomy following CCRT, with particular focus on non-complete responders (non-CR).
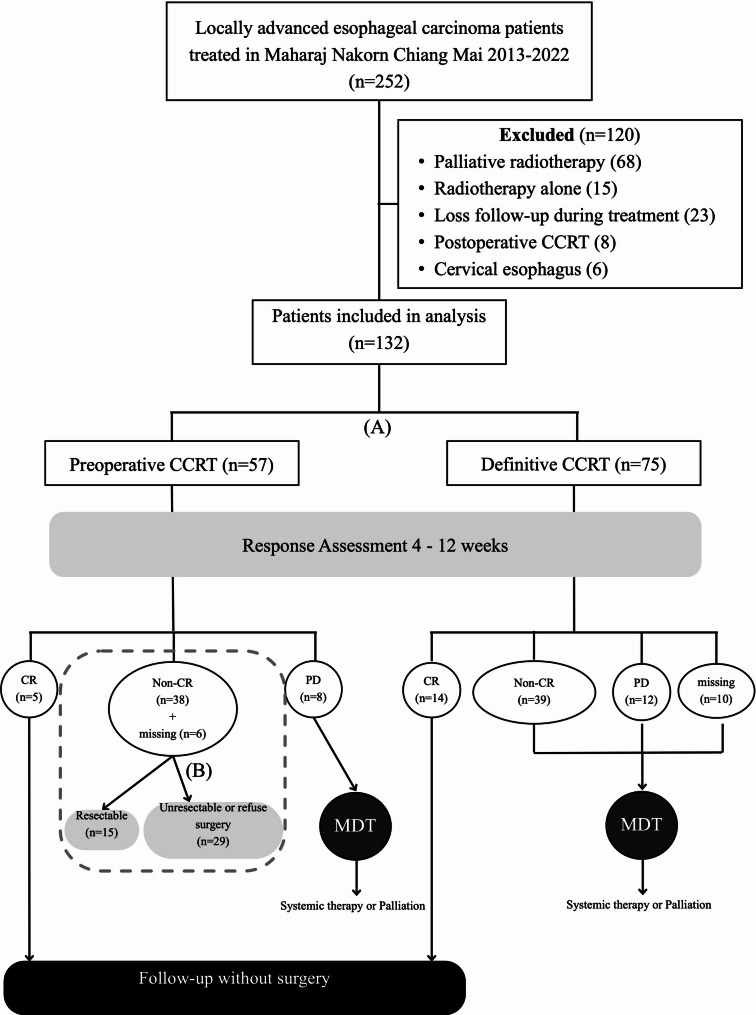
Methods: We conducted a retrospective cohort study of 132 patients with locally advanced esophageal cancer treated at Maharaj Nakorn Chiang Mai Hospital between 2013 and 2022. Patients were categorized based on initial treatment into preoperative CCRT or definitive CCRT groups. Overall survival (OS) and progression-free survival (PFS) were compared using multivariable Cox regression. A secondary analysis stratified patients into three groups by clinical response and surgical status: CR without surgery, non-CR with surgery, and non-CR without surgery. To reduce baseline imbalances and selection bias, inverse probability of treatment weighting (IPTW) was applied in the non-CR subgroup initially intended for preoperative CCRT.
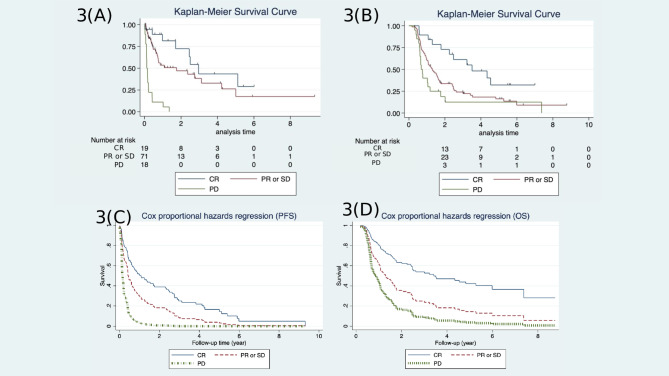
Results: Baseline characteristics were balanced except for tumor location. Median follow-up was 1.23 years (IQR: 0.64-2.50). Overall, 1-/2-year PFS was 27.97%/17.80%, while OS was 60.47%/37.33%. Median survival did not differ between preoperative versus definitive CCRT (1.20 vs. 1.52 years, p = 0.346). However, in the surgical-status analysis, patients undergoing post-CCRT esophagectomy showed significantly improved PFS and OS versus non-surgical non-CR patients (PFS HR: 2.89, p < 0.001; OS HR: 2.97, p = 0.001). Notably, surgical non-CR patients achieved OS comparable to CR patients without esophagectomy (HR: 1.12, p = 0.812). To minimize selection bias, we conducted an IPTW-adjusted analysis in the subgroup of non-CR patients initially assigned to preoperative CCRT. After IPTW, the survival benefit of surgery remained significant, with improved PFS (HR: 3.75; 95% CI: 1.40-10.08; p = 0.009) and OS (HR: 2.74; 95% CI: 1.57-4.77; p < 0.001) compared to CCRT alone.
Conclusion: Esophagectomy after CCRT provides survival benefits equivalent to achieving CR with CCRT alone, particularly for non-CR patients. These results advocate for surgical integration as a salvage strategy for incomplete responders in locally advanced esophageal cancer.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


