Therapeutic outcomes and predictors of efficacy for endoscopic variceal ligation plus propranolol in liver cirrhosis-related upper gastrointestinal bleeding.
{"title":"Therapeutic outcomes and predictors of efficacy for endoscopic variceal ligation plus propranolol in liver cirrhosis-related upper gastrointestinal bleeding.","authors":"Dan-Feng Gong, Long Cheng","doi":"10.4240/wjgs.v17.i9.109152","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cirrhosis-related upper gastrointestinal bleeding (UGIB) poses a fatal risk, and endoscopic ligation as a sole intervention shows inadequate effectiveness.</p><p><strong>Aim: </strong>To evaluate the therapeutic efficacy of endoscopic variceal ligation (EVL) plus propranolol <i>vs</i> EVL monotherapy in patients with cirrhosis complicated with acute UGIB and identify predictors for clinical outcomes.</p><p><strong>Methods: </strong>This study enrolled 99 consecutive patients with cirrhosis presenting with acute UGIB between January 2024 and January 2025. Participants were allocated to either the control group (<i>n</i> = 49) receiving EVL alone or (2) the research group (<i>n</i> = 50) receiving EVL plus propranolol. Primary outcomes included treatment efficacy, venous blood flow [portal venous flow (PVF)/splenic venous flow (SVF)], and postoperative outcomes (hemostasis time, length of hospital stay, and rebleeding rates). Univariate and multivariate regression analyses were conducted to determine independent predictors of treatment response.</p><p><strong>Results: </strong>Compared with the control group, the research group demonstrated significantly better outcomes, including higher overall treatment efficacy, greater reductions in PVF and SVF, shorter hemostasis time and hospital stay, and lower rebleeding rates. Univariate analysis demonstrated significant associations between treatment efficacy and age, cirrhosis duration, Child-Pugh grade, bleeding duration, and treatment approach in patients with cirrhosis complicated with acute UGIB. Multivariate logistic regression identified three independent risk factors for poor outcomes, namely, advanced age (> 55 years), prolonged cirrhosis duration (≥ 4 years), and delayed bleeding intervention (> 24 hours).</p><p><strong>Conclusion: </strong>The EVL plus propranolol regimen demonstrates significant efficacy in treating UGIB in cirrhosis, outperforming EVL alone in improving hemodynamics (PVF/SVF), shortening hemostasis and hospitalization duration, and reducing rebleeding rates. Moreover, advanced age, prolonged disease duration, and longer bleeding times are independent risk factors for poor therapeutic outcomes.</p>","PeriodicalId":23759,"journal":{"name":"World Journal of Gastrointestinal Surgery","volume":"17 9","pages":"109152"},"PeriodicalIF":1.7000,"publicationDate":"2025-09-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476765/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4240/wjgs.v17.i9.109152","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cirrhosis-related upper gastrointestinal bleeding (UGIB) poses a fatal risk, and endoscopic ligation as a sole intervention shows inadequate effectiveness.
Aim: To evaluate the therapeutic efficacy of endoscopic variceal ligation (EVL) plus propranolol vs EVL monotherapy in patients with cirrhosis complicated with acute UGIB and identify predictors for clinical outcomes.
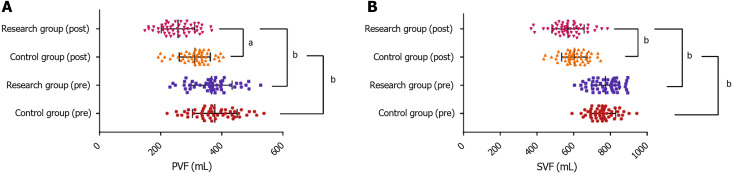
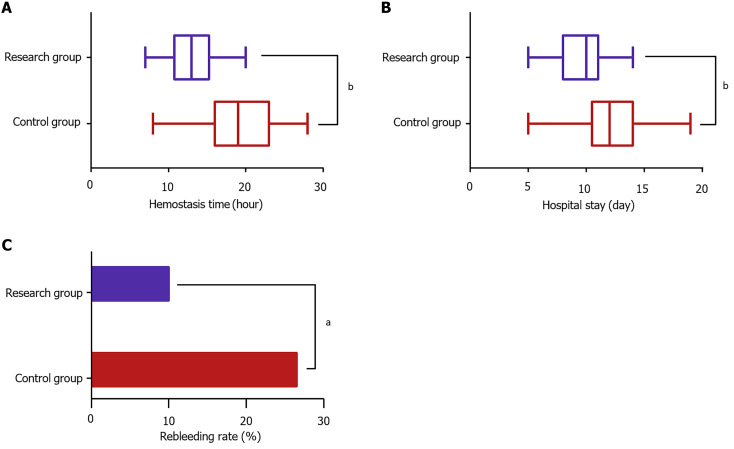
Methods: This study enrolled 99 consecutive patients with cirrhosis presenting with acute UGIB between January 2024 and January 2025. Participants were allocated to either the control group (n = 49) receiving EVL alone or (2) the research group (n = 50) receiving EVL plus propranolol. Primary outcomes included treatment efficacy, venous blood flow [portal venous flow (PVF)/splenic venous flow (SVF)], and postoperative outcomes (hemostasis time, length of hospital stay, and rebleeding rates). Univariate and multivariate regression analyses were conducted to determine independent predictors of treatment response.
Results: Compared with the control group, the research group demonstrated significantly better outcomes, including higher overall treatment efficacy, greater reductions in PVF and SVF, shorter hemostasis time and hospital stay, and lower rebleeding rates. Univariate analysis demonstrated significant associations between treatment efficacy and age, cirrhosis duration, Child-Pugh grade, bleeding duration, and treatment approach in patients with cirrhosis complicated with acute UGIB. Multivariate logistic regression identified three independent risk factors for poor outcomes, namely, advanced age (> 55 years), prolonged cirrhosis duration (≥ 4 years), and delayed bleeding intervention (> 24 hours).
Conclusion: The EVL plus propranolol regimen demonstrates significant efficacy in treating UGIB in cirrhosis, outperforming EVL alone in improving hemodynamics (PVF/SVF), shortening hemostasis and hospitalization duration, and reducing rebleeding rates. Moreover, advanced age, prolonged disease duration, and longer bleeding times are independent risk factors for poor therapeutic outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


