Aarushi Gupta, Tinatin Chikhradze, Afrah Arshad, Rahmah Ashar Sakrani, Zainab Khan, Melake Getahun, Samreen Rizwan Ahmed Shaikh, Wajiha Syed, Tanish Baweja, Abhijith Remesan, Cheryl Lewis, Joy Doshi, Muneeb Khawar, Asraf Hussain, Muhammad Muneeb Khawar
{"title":"Partial upper sternotomy <i>vs</i> full median sternotomy in obese patients undergoing aortic valve replacement: A meta-analysis.","authors":"Aarushi Gupta, Tinatin Chikhradze, Afrah Arshad, Rahmah Ashar Sakrani, Zainab Khan, Melake Getahun, Samreen Rizwan Ahmed Shaikh, Wajiha Syed, Tanish Baweja, Abhijith Remesan, Cheryl Lewis, Joy Doshi, Muneeb Khawar, Asraf Hussain, Muhammad Muneeb Khawar","doi":"10.4330/wjc.v17.i9.110838","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Obese patients (body mass index ≥ 30 kg/m²) undergoing isolated aortic valve replacement (AVR) face increased surgical risks due to comorbidities. Partial upper sternotomy (PUS), a minimally invasive approach, may reduce complications compared to full median sternotomy (FMS). We hypothesize that PUS improves outcomes over FMS in obese patients undergoing AVR.</p><p><strong>Aim: </strong>To compare the efficacy and safety of PUS <i>vs</i> FMS in obese patients undergoing isolated AVR.</p><p><strong>Methods: </strong>This systematic review and meta-analysis followed PRISMA guidelines, searching PubMed, EMBASE, and Cochrane databases for observational studies comparing PUS <i>vs</i> FMS in obese patients undergoing AVR. Outcomes were analyzed using odds ratios (OR), mean differences (MD), 95% confidence intervals (CI), <i>I</i>² statistic, and Newcastle-Ottawa Scale was used for quality assessment.</p><p><strong>Results: </strong>Four observational studies involving 677 patients were analyzed. PUS reduced intensive care unit stay (MD -2.67 days, 95%CI: -4.43 to -0.90, <i>P</i> = 0.003, <i>I</i>² = 78%) but increased cardiopulmonary bypass time (MD 5.62 minutes, 95%CI: -0.36 to 11.59, <i>I</i>² = 55%). No differences were observed in renal failure (OR 1.13, 95%CI: 0.63-2.94, <i>I</i>² = 0%), atrial fibrillation (OR 0.81, 95%CI: 0.43-1.54, <i>I</i>² = 30%), reexploration (OR 1.09, 95%CI: 0.48-2.47, <i>I</i>² = 0%), postoperative bleeding (OR 1.48, 95%CI: 0.53-4.15, <i>I</i>² = 60%), wound infection (OR 1.23, 95%CI: 0.70-2.14, <i>I</i>² = 0%), hospital stay (MD 0.51 days, 95%CI: -4.13 to 5.15, <i>I</i>² = 90%), or cross-clamp time (MD 4.03 minutes, 95%CI: -0.75 to 8.80, <i>I</i>² = 50%).</p><p><strong>Conclusion: </strong>PUS is safe and effective for obese patients undergoing AVR, reducing intensive care unit stay and enhancing recovery, provided surgical expertise is available.</p>","PeriodicalId":23800,"journal":{"name":"World Journal of Cardiology","volume":"17 9","pages":"110838"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476599/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4330/wjc.v17.i9.110838","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Obese patients (body mass index ≥ 30 kg/m²) undergoing isolated aortic valve replacement (AVR) face increased surgical risks due to comorbidities. Partial upper sternotomy (PUS), a minimally invasive approach, may reduce complications compared to full median sternotomy (FMS). We hypothesize that PUS improves outcomes over FMS in obese patients undergoing AVR.
Aim: To compare the efficacy and safety of PUS vs FMS in obese patients undergoing isolated AVR.
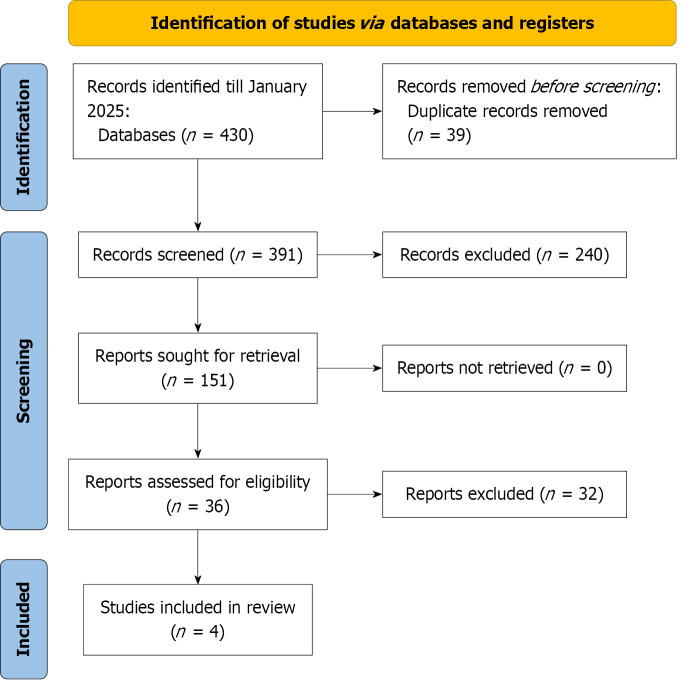
Methods: This systematic review and meta-analysis followed PRISMA guidelines, searching PubMed, EMBASE, and Cochrane databases for observational studies comparing PUS vs FMS in obese patients undergoing AVR. Outcomes were analyzed using odds ratios (OR), mean differences (MD), 95% confidence intervals (CI), I² statistic, and Newcastle-Ottawa Scale was used for quality assessment.
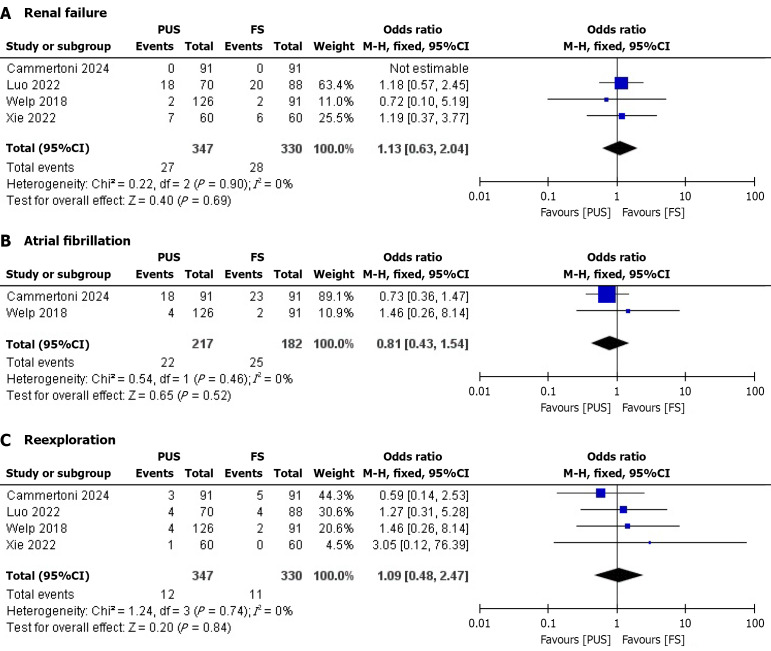
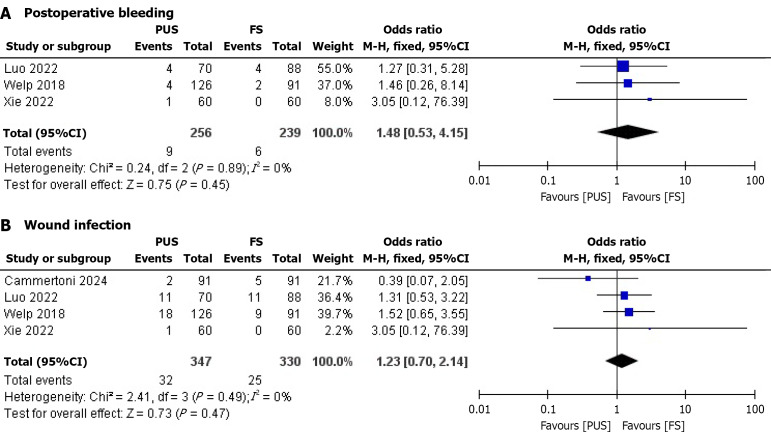
Results: Four observational studies involving 677 patients were analyzed. PUS reduced intensive care unit stay (MD -2.67 days, 95%CI: -4.43 to -0.90, P = 0.003, I² = 78%) but increased cardiopulmonary bypass time (MD 5.62 minutes, 95%CI: -0.36 to 11.59, I² = 55%). No differences were observed in renal failure (OR 1.13, 95%CI: 0.63-2.94, I² = 0%), atrial fibrillation (OR 0.81, 95%CI: 0.43-1.54, I² = 30%), reexploration (OR 1.09, 95%CI: 0.48-2.47, I² = 0%), postoperative bleeding (OR 1.48, 95%CI: 0.53-4.15, I² = 60%), wound infection (OR 1.23, 95%CI: 0.70-2.14, I² = 0%), hospital stay (MD 0.51 days, 95%CI: -4.13 to 5.15, I² = 90%), or cross-clamp time (MD 4.03 minutes, 95%CI: -0.75 to 8.80, I² = 50%).
Conclusion: PUS is safe and effective for obese patients undergoing AVR, reducing intensive care unit stay and enhancing recovery, provided surgical expertise is available.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


