{"title":"Survival benefit of primary tumor resection in pancreatic neuroendocrine tumors with unresectable liver metastases: A meta-analysis.","authors":"Jie Gong, Ben-Jian Gao, Ze-Hua Lei","doi":"10.4240/wjgs.v17.i9.107966","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pancreatic neuroendocrine tumors (PNETs) are rare malignancies frequently associated with liver metastases (LM). The benefit of primary tumor resection (PTR) in patients with unresectable LM remains controversial. This study evaluates the impact of PTR on overall survival (OS) and tumor grading by integrating evidence from a systematic review, meta-analysis, and Surveillance, Epidemiology, and End Results (SEER) database analysis.</p><p><strong>Aim: </strong>To evaluate the survival benefits of PTR in patients with PNETs and LM.</p><p><strong>Methods: </strong>This study was conducted in accordance with the PRISMA guidelines. A systematic literature search and meta-analysis were performed using five databases: PubMed, Web of Science, EMBASE, Cochrane Library, and CNKI, with records included up to February 2025. A total of 16 studies (<i>n</i> = 8761; including 1 prospective and 15 retrospective studies) were included. A random-effects model was applied to pool hazard ratios for OS and odds ratios for tumor grading, with heterogeneity assessed by the <i>I</i> <sup>2</sup> statistic. Risk of bias was evaluated using the ROBINS-I tool. In addition, an independent analysis based on the SEER database (<i>n</i> = 791) was conducted using Kaplan-Meier survival curves and log-rank tests.</p><p><strong>Results: </strong>Meta-analysis results revealed that PTR significantly improved OS in patients with PNETs and LM (hazard ratio = -1.10, 95% confidence interval: -1.43 to -0.71, <i>P</i> < 0.0001). Subgroup analyses showed that neither study design (prospective vs. retrospective) nor sample size (< 400 <i>vs</i> ≥ 400) significantly influenced the survival benefit. In terms of tumor grading, no statistically significant difference was observed between the surgical and non-surgical groups (odds ratio = 1.60, 95% confidence interval: 0.70-3.63, <i>P</i> = 0.26). Independent analysis of the SEER database (<i>n</i> = 791) further confirmed the survival advantage of PTR across different tumor differentiation levels, with significant differences in OS between surgical and non-surgical groups (<i>P</i> < 0.05).</p><p><strong>Conclusion: </strong>PTR significantly improves OS in PNET patients with LM. However, its effect on tumor grading remains unclear, warranting further prospective studies to refine surgical strategies for this population.</p>","PeriodicalId":23759,"journal":{"name":"World Journal of Gastrointestinal Surgery","volume":"17 9","pages":"107966"},"PeriodicalIF":1.7000,"publicationDate":"2025-09-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476756/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4240/wjgs.v17.i9.107966","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Pancreatic neuroendocrine tumors (PNETs) are rare malignancies frequently associated with liver metastases (LM). The benefit of primary tumor resection (PTR) in patients with unresectable LM remains controversial. This study evaluates the impact of PTR on overall survival (OS) and tumor grading by integrating evidence from a systematic review, meta-analysis, and Surveillance, Epidemiology, and End Results (SEER) database analysis.
Aim: To evaluate the survival benefits of PTR in patients with PNETs and LM.
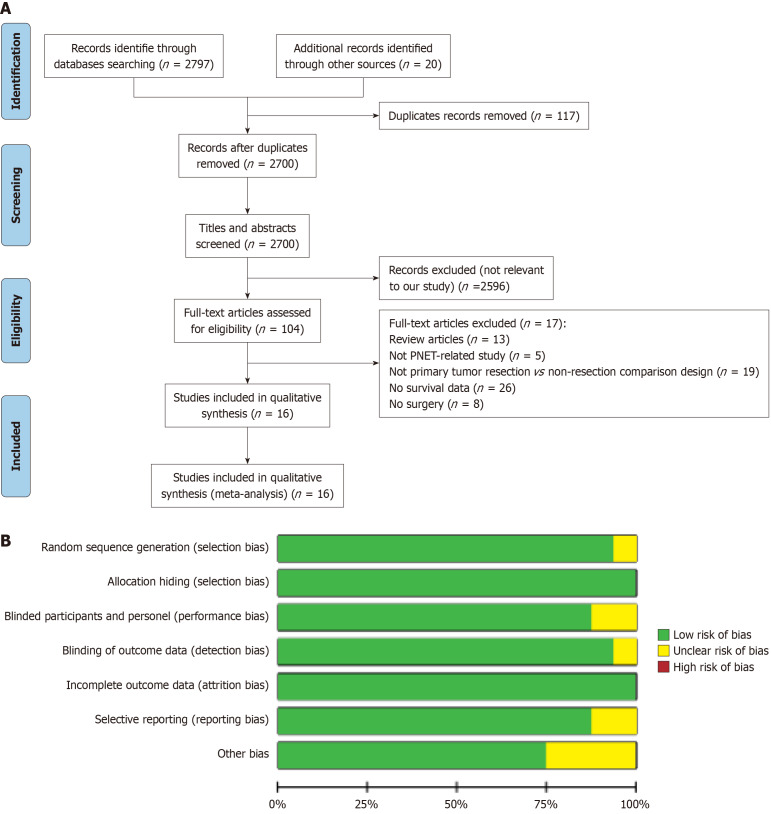
Methods: This study was conducted in accordance with the PRISMA guidelines. A systematic literature search and meta-analysis were performed using five databases: PubMed, Web of Science, EMBASE, Cochrane Library, and CNKI, with records included up to February 2025. A total of 16 studies (n = 8761; including 1 prospective and 15 retrospective studies) were included. A random-effects model was applied to pool hazard ratios for OS and odds ratios for tumor grading, with heterogeneity assessed by the I2 statistic. Risk of bias was evaluated using the ROBINS-I tool. In addition, an independent analysis based on the SEER database (n = 791) was conducted using Kaplan-Meier survival curves and log-rank tests.
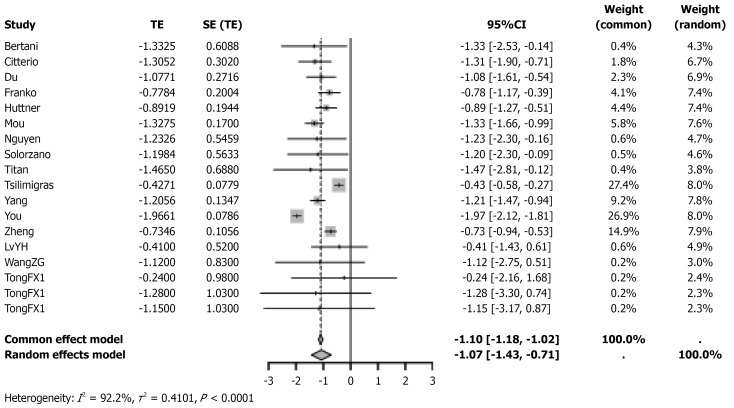
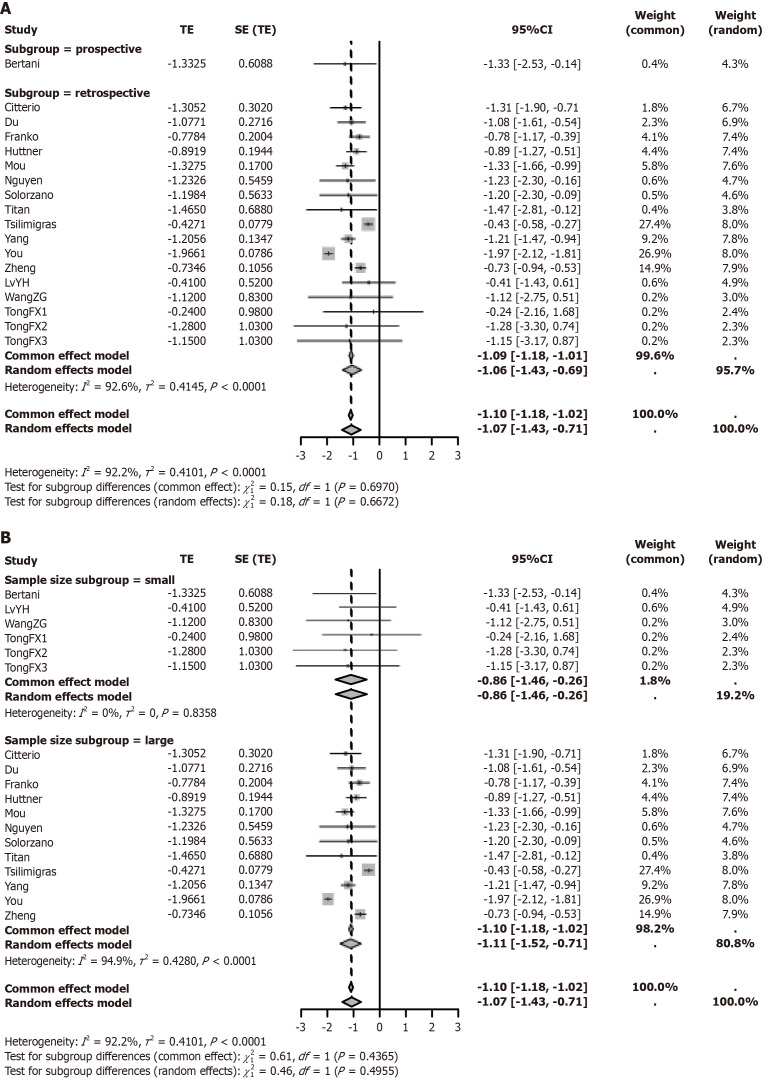
Results: Meta-analysis results revealed that PTR significantly improved OS in patients with PNETs and LM (hazard ratio = -1.10, 95% confidence interval: -1.43 to -0.71, P < 0.0001). Subgroup analyses showed that neither study design (prospective vs. retrospective) nor sample size (< 400 vs ≥ 400) significantly influenced the survival benefit. In terms of tumor grading, no statistically significant difference was observed between the surgical and non-surgical groups (odds ratio = 1.60, 95% confidence interval: 0.70-3.63, P = 0.26). Independent analysis of the SEER database (n = 791) further confirmed the survival advantage of PTR across different tumor differentiation levels, with significant differences in OS between surgical and non-surgical groups (P < 0.05).
Conclusion: PTR significantly improves OS in PNET patients with LM. However, its effect on tumor grading remains unclear, warranting further prospective studies to refine surgical strategies for this population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


