{"title":"Paediatric Sinogenic Subdural and Extradural Empyema: A Review of Local Surgical Management Over 10 Years.","authors":"David McCrory, Grigoris Iosif, Keith Trimble","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To investigate timing and surgical approaches of multidisciplinary management of sinogenic subdural and extradural empyema in the paediatric population.</p><p><strong>Methods: </strong>We performed a retrospective analysis of all cases of sinogenic subdural and extradural empyema at our tertiary referral centre over a 10-year study period from 1<sup>st</sup> May 2012 to 1<sup>st</sup> May 2022. Data on demographics, presenting features, surgical management, length of stay, radiological investigations, microbiology results and long-term morbidity was recorded in a spreadsheet for analysis.</p><p><strong>Results: </strong>We identified 11 children (mean age 11.3 years ± 2.3). In this sample, 7 were male (63.6%) and 4 female (36.4%). There were 7 cases of subdural empyema (63.6%), 2 cases of extradural empyema (18.2%) and 2 cases with both subdural and extradural empyema (18.2%). There were significant underlying co-morbidities in 2 cases (18%). The frontal sinus was suspected source in 10 cases (91%). Endoscopic sinus surgery was performed in 10 cases (91%); with 9 of these cases (90%) as/with the initial operation or within 24 hours of initial operation. Craniotomy was required in 9 cases total (81%), with 5 cases (56%) as/with the initial operation or within 24 hours of initial operation. After initial craniotomy 4 cases (44%) required further neurosurgical evacuation of abscess. Additionally, 2 cases managed with initial burrhole later required craniotomy. All 3 cases of small volume subdural empyema without neurological deficit were initially managed with endoscopic sinus surgery only and all cases subsequently required craniotomy. All cases with subdural empyema required craniotomy (n=9) whereas all cases with isolated extradural empyema avoided craniotomy (n=2). There was a longer length of stay in those that presented with neurology or low GCS than those that did not (27 days ± 10 compared to 86 days ± 41, p= 0.009). Long term morbidity and repeated neurosurgical intervention were more common in those cases with subdural empyema than those without subdural empyema, (55% vs 0% and 67% vs 0% respectively) although only 2 patients did not have subdural empyema (no statistical analysis available given small numbers). A Streptococcus milleri group microbe was isolated in 82% of cases.</p><p><strong>Conclusions: </strong>Endoscopic sinus surgery does not seem effective at preventing the need for craniotomy in cases of subdural empyema. It does have a role in aiding microbiological diagnosis. ESS may have a role in the treatment of extradural empyema and avoiding craniotomy. Subdural empyema has a higher morbidity and return to theatre rate than extradural empyema. Those that present with a neurological deficit or decreased GCS have a longer length of stay. Larger studies are required to assess the timing and extent of surgical interventions for subdural and extradural empyema.</p>","PeriodicalId":94250,"journal":{"name":"The Ulster medical journal","volume":"94 2","pages":"83-88"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476120/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Ulster medical journal","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To investigate timing and surgical approaches of multidisciplinary management of sinogenic subdural and extradural empyema in the paediatric population.
Methods: We performed a retrospective analysis of all cases of sinogenic subdural and extradural empyema at our tertiary referral centre over a 10-year study period from 1st May 2012 to 1st May 2022. Data on demographics, presenting features, surgical management, length of stay, radiological investigations, microbiology results and long-term morbidity was recorded in a spreadsheet for analysis.
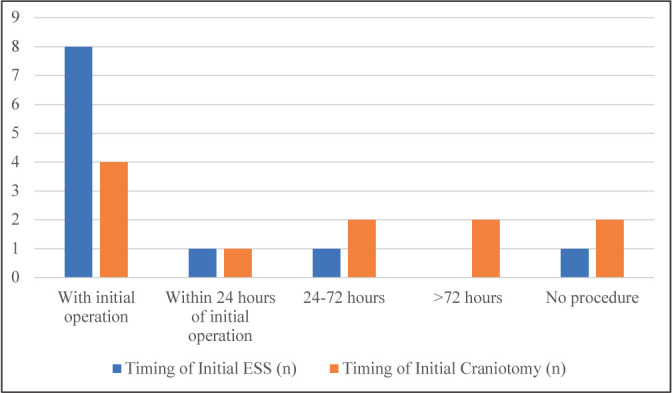
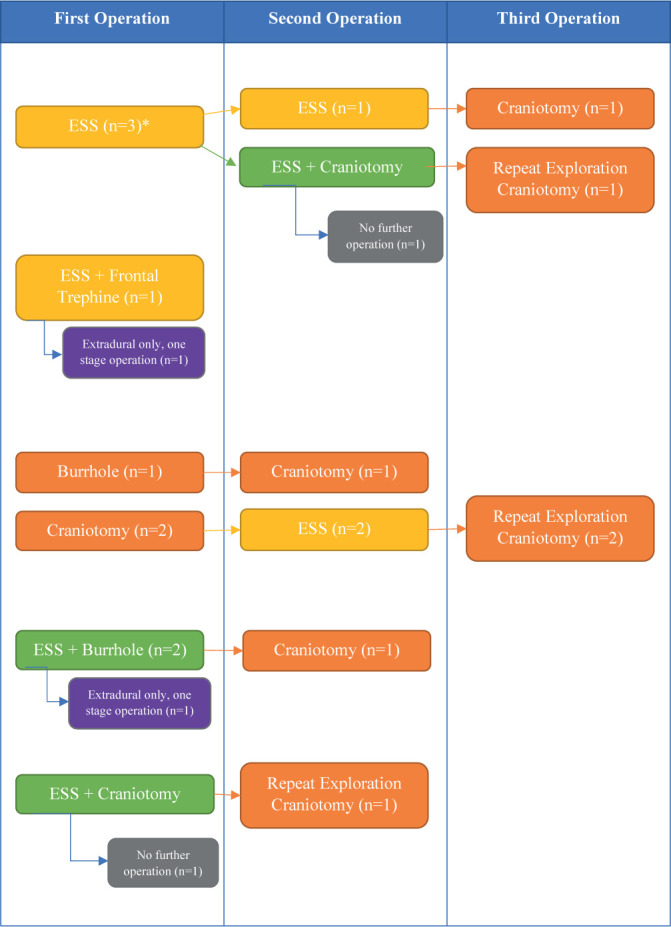
Results: We identified 11 children (mean age 11.3 years ± 2.3). In this sample, 7 were male (63.6%) and 4 female (36.4%). There were 7 cases of subdural empyema (63.6%), 2 cases of extradural empyema (18.2%) and 2 cases with both subdural and extradural empyema (18.2%). There were significant underlying co-morbidities in 2 cases (18%). The frontal sinus was suspected source in 10 cases (91%). Endoscopic sinus surgery was performed in 10 cases (91%); with 9 of these cases (90%) as/with the initial operation or within 24 hours of initial operation. Craniotomy was required in 9 cases total (81%), with 5 cases (56%) as/with the initial operation or within 24 hours of initial operation. After initial craniotomy 4 cases (44%) required further neurosurgical evacuation of abscess. Additionally, 2 cases managed with initial burrhole later required craniotomy. All 3 cases of small volume subdural empyema without neurological deficit were initially managed with endoscopic sinus surgery only and all cases subsequently required craniotomy. All cases with subdural empyema required craniotomy (n=9) whereas all cases with isolated extradural empyema avoided craniotomy (n=2). There was a longer length of stay in those that presented with neurology or low GCS than those that did not (27 days ± 10 compared to 86 days ± 41, p= 0.009). Long term morbidity and repeated neurosurgical intervention were more common in those cases with subdural empyema than those without subdural empyema, (55% vs 0% and 67% vs 0% respectively) although only 2 patients did not have subdural empyema (no statistical analysis available given small numbers). A Streptococcus milleri group microbe was isolated in 82% of cases.
Conclusions: Endoscopic sinus surgery does not seem effective at preventing the need for craniotomy in cases of subdural empyema. It does have a role in aiding microbiological diagnosis. ESS may have a role in the treatment of extradural empyema and avoiding craniotomy. Subdural empyema has a higher morbidity and return to theatre rate than extradural empyema. Those that present with a neurological deficit or decreased GCS have a longer length of stay. Larger studies are required to assess the timing and extent of surgical interventions for subdural and extradural empyema.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


