Shunsuke Todani, Kazuhiro Shimizu, Shuji Sato, Kohji Shirai, Atsuhito Saiki
{"title":"Association Between Longitudinal Changes in Cardio-Ankle Vascular Index and Aortic Stenosis Progression in Dialysis Patients: A Retrospective Study.","authors":"Shunsuke Todani, Kazuhiro Shimizu, Shuji Sato, Kohji Shirai, Atsuhito Saiki","doi":"10.7759/cureus.93263","DOIUrl":null,"url":null,"abstract":"<p><p>Objective In dialysis patients, echocardiography often underestimates the progression of aortic stenosis (AS) due to blood pressure fluctuations and extensive calcification that obscure standard indices. We evaluated whether serial changes in the cardio-ankle vascular index (CAVI), a blood pressure-independent marker of arterial stiffness, can anticipate severe AS and guide the timing of valve replacement. Methods This single-center, retrospective study screened 1,169 maintenance dialysis patients (2015-2023). Forty-one patients who underwent surgical or transcatheter aortic valve replacement (AVR/TAVR) had valid CAVI measurements at four time points: 2 years and 1 year before surgery, immediately before surgery, and 1 year after surgery. The -2-year time point served as the baseline. Hemodynamic, echocardiographic, and laboratory data were analyzed using the Friedman and Wilcoxon tests. Severe AS progression was defined as a new mean pressure gradient (meanPG) ≥ 40 mmHg. Determinants of progression were identified using multivariable logistic regression. Results Median CAVI declined from 10.2 to 9.4 over the two years preceding surgery (p < 0.001) and rose to 11.1 one year post-AVR/TAVR (p < 0.001). Simultaneously, ejection time increased, ejection fraction decreased, and Vmax, maxPG, stroke volume, and stroke volume index (SVi) all rose significantly (p < 0.01 for each), with no significant changes in blood pressure or heart rate. Patients who progressed to severe AS showed a greater CAVI decline (ΔCAVI -2.90 vs. -0.67; p = 0.022) and higher Vmax (4.0 vs. 3.0 m/s; p < 0.001). ΔCAVI was the only independent predictor of severe AS progression (OR 0.51 per 1-unit decrease; 95% CI: 0.20-0.89; p = 0.013). Age and sex were not significant. CAVI and peak PG showed a modest inverse correlation (ρ = -0.35). Conclusion In dialysis patients, a marked preoperative decline in CAVI nearly doubles the risk of emergent severe AS and normalizes after valve replacement, indicating true hemodynamic responsiveness. Serial CAVI monitoring, simple, noninvasive, and reproducible, may offer an early warning signal and help optimize intervention timing when echocardiographic findings are ambiguous.</p>","PeriodicalId":93960,"journal":{"name":"Cureus","volume":"17 9","pages":"e93263"},"PeriodicalIF":1.3000,"publicationDate":"2025-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12465358/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cureus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7759/cureus.93263","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
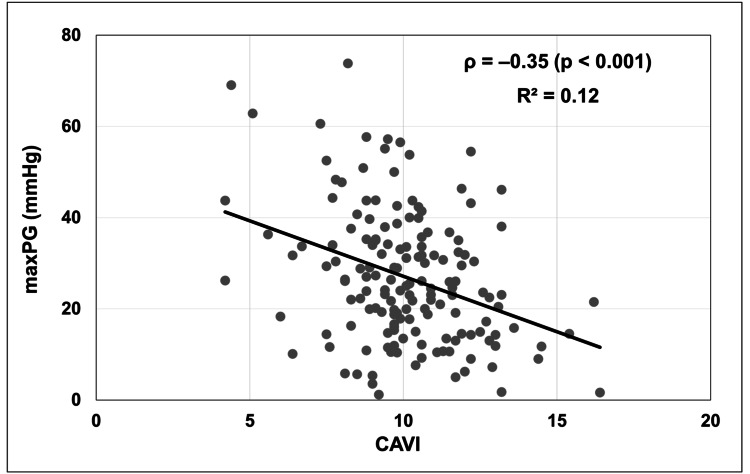
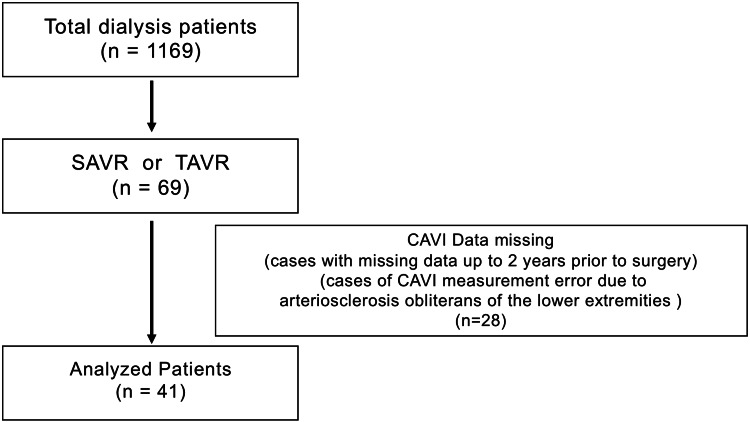
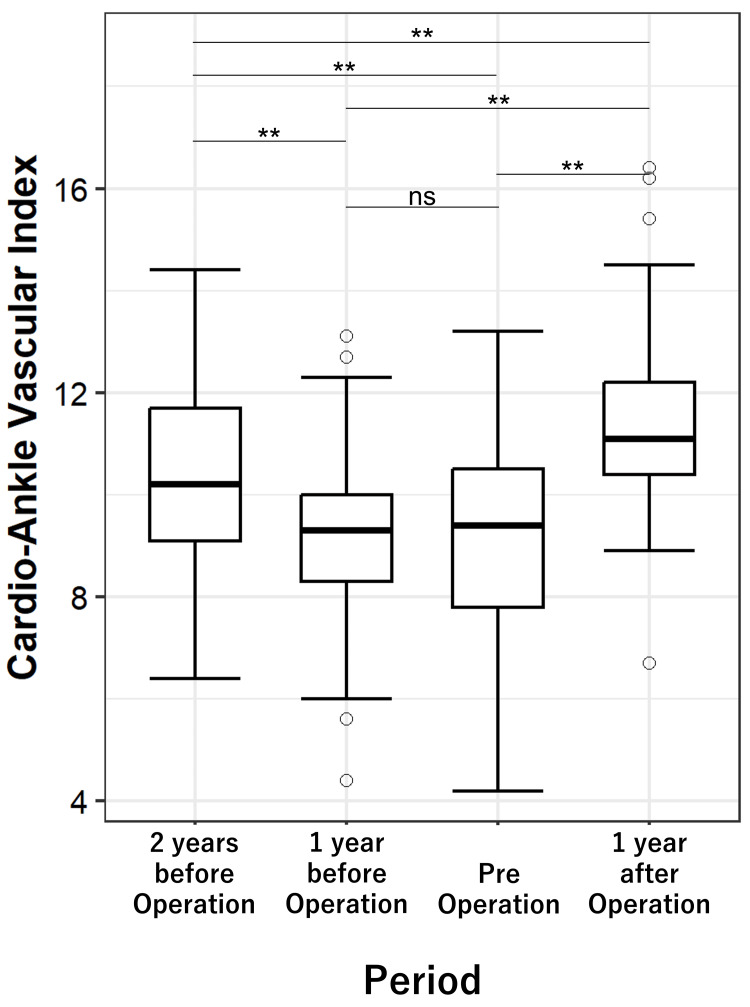
Objective In dialysis patients, echocardiography often underestimates the progression of aortic stenosis (AS) due to blood pressure fluctuations and extensive calcification that obscure standard indices. We evaluated whether serial changes in the cardio-ankle vascular index (CAVI), a blood pressure-independent marker of arterial stiffness, can anticipate severe AS and guide the timing of valve replacement. Methods This single-center, retrospective study screened 1,169 maintenance dialysis patients (2015-2023). Forty-one patients who underwent surgical or transcatheter aortic valve replacement (AVR/TAVR) had valid CAVI measurements at four time points: 2 years and 1 year before surgery, immediately before surgery, and 1 year after surgery. The -2-year time point served as the baseline. Hemodynamic, echocardiographic, and laboratory data were analyzed using the Friedman and Wilcoxon tests. Severe AS progression was defined as a new mean pressure gradient (meanPG) ≥ 40 mmHg. Determinants of progression were identified using multivariable logistic regression. Results Median CAVI declined from 10.2 to 9.4 over the two years preceding surgery (p < 0.001) and rose to 11.1 one year post-AVR/TAVR (p < 0.001). Simultaneously, ejection time increased, ejection fraction decreased, and Vmax, maxPG, stroke volume, and stroke volume index (SVi) all rose significantly (p < 0.01 for each), with no significant changes in blood pressure or heart rate. Patients who progressed to severe AS showed a greater CAVI decline (ΔCAVI -2.90 vs. -0.67; p = 0.022) and higher Vmax (4.0 vs. 3.0 m/s; p < 0.001). ΔCAVI was the only independent predictor of severe AS progression (OR 0.51 per 1-unit decrease; 95% CI: 0.20-0.89; p = 0.013). Age and sex were not significant. CAVI and peak PG showed a modest inverse correlation (ρ = -0.35). Conclusion In dialysis patients, a marked preoperative decline in CAVI nearly doubles the risk of emergent severe AS and normalizes after valve replacement, indicating true hemodynamic responsiveness. Serial CAVI monitoring, simple, noninvasive, and reproducible, may offer an early warning signal and help optimize intervention timing when echocardiographic findings are ambiguous.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


