{"title":"Central venous pressure dynamics in neonates with hypoxic-ischemic encephalopathy: insights into high mean airway pressure, PPHN, and ECMO management.","authors":"Tomonori Kurimoto, Tokuhisa Takuya, Masaya Kibe, Toshio Harumatsu, Hiroshi Ohashi, Tsuyoshi Yamamoto, Eiji Hirakawa","doi":"10.3389/fped.2025.1611740","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Central venous pressure (CVP) monitoring provides valuable insights into hemodynamic changes; however, its application in neonates with hypoxic-ischemic encephalopathy (HIE) undergoing advanced therapies remains underexplored. This study aimed to evaluate the dynamics of CVP under varying conditions, including high mean airway pressure (MAP), persistent pulmonary hypertension of the newborn (PPHN), and treatment with inhaled nitric oxide (iNO) and extracorporeal membrane oxygenation (ECMO).</p><p><strong>Methods: </strong>This retrospective study included 18 neonates diagnosed with HIE, who received brain hypothermia therapy and had umbilical venous catheters (UVC) appropriately placed for CVP monitoring. CVP values were analyzed in relation to high MAP (≥10 cmH₂O), PPHN status, and pre- and post-therapeutic interventions such as iNO and ECMO. Statistical comparisons were performed using Mann-Whitney <i>U</i> tests for continuous variables, with significance set at <i>p</i> < 0.05.</p><p><strong>Results: </strong>Neonates in the high MAP group exhibited significantly higher mean CVP values than those in the normal MAP group (6 vs. 5 mmHg, <i>p</i> = 0.03). In the PPHN + high MAP group, the mean CVP, oxygenation index, and FiO₂ levels were markedly elevated compared with the high MAP group without PPHN. iNO administration significantly reduced the mean CVP (7 mmHg pre-iNO vs. 4 mmHg post-iNO, <i>p</i> = 0.04), whereas VV-ECMO initiation resulted in an increased CVP (mean CVP: 8 mmHg pre-ECMO vs. 13 mmHg post-ECMO, <i>p</i> = 0.03).</p><p><strong>Discussion: </strong>CVP monitoring via UVC provides critical information on hemodynamic changes in neonates with HIE, particularly under high MAP and PPHN conditions. While iNO effectively reduced CVP and improved oxygenation, VV-ECMO led to elevated CVP, likely due to the return cannula flow. These findings underscore the need for optimized cannula placement and ventilatory strategies to minimize hemodynamic instability during advanced neonatal therapy.</p>","PeriodicalId":12637,"journal":{"name":"Frontiers in Pediatrics","volume":"13 ","pages":"1611740"},"PeriodicalIF":2.0000,"publicationDate":"2025-09-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12460447/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Pediatrics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fped.2025.1611740","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Central venous pressure (CVP) monitoring provides valuable insights into hemodynamic changes; however, its application in neonates with hypoxic-ischemic encephalopathy (HIE) undergoing advanced therapies remains underexplored. This study aimed to evaluate the dynamics of CVP under varying conditions, including high mean airway pressure (MAP), persistent pulmonary hypertension of the newborn (PPHN), and treatment with inhaled nitric oxide (iNO) and extracorporeal membrane oxygenation (ECMO).
Methods: This retrospective study included 18 neonates diagnosed with HIE, who received brain hypothermia therapy and had umbilical venous catheters (UVC) appropriately placed for CVP monitoring. CVP values were analyzed in relation to high MAP (≥10 cmH₂O), PPHN status, and pre- and post-therapeutic interventions such as iNO and ECMO. Statistical comparisons were performed using Mann-Whitney U tests for continuous variables, with significance set at p < 0.05.
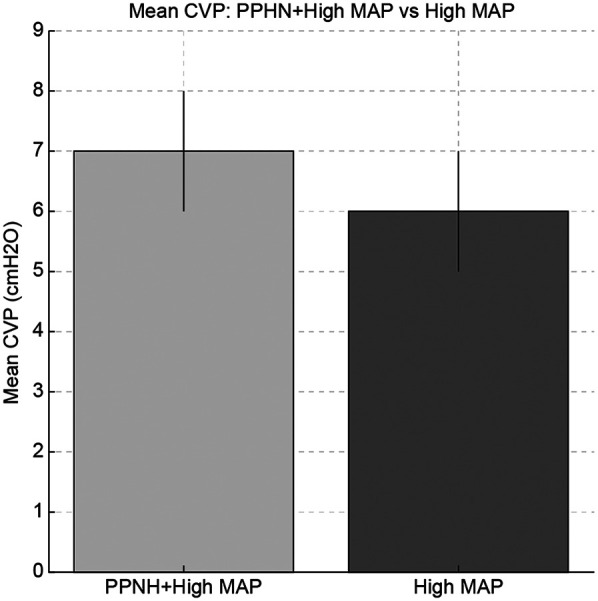
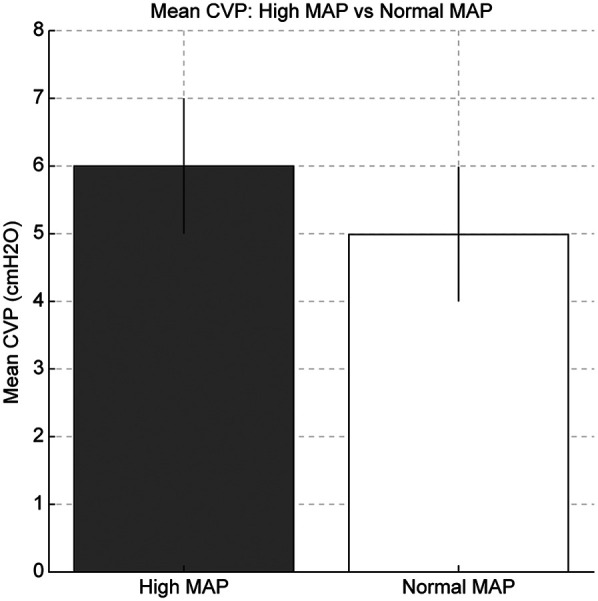
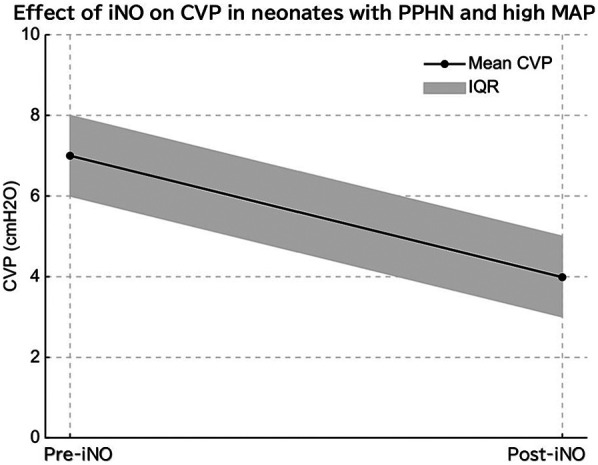
Results: Neonates in the high MAP group exhibited significantly higher mean CVP values than those in the normal MAP group (6 vs. 5 mmHg, p = 0.03). In the PPHN + high MAP group, the mean CVP, oxygenation index, and FiO₂ levels were markedly elevated compared with the high MAP group without PPHN. iNO administration significantly reduced the mean CVP (7 mmHg pre-iNO vs. 4 mmHg post-iNO, p = 0.04), whereas VV-ECMO initiation resulted in an increased CVP (mean CVP: 8 mmHg pre-ECMO vs. 13 mmHg post-ECMO, p = 0.03).
Discussion: CVP monitoring via UVC provides critical information on hemodynamic changes in neonates with HIE, particularly under high MAP and PPHN conditions. While iNO effectively reduced CVP and improved oxygenation, VV-ECMO led to elevated CVP, likely due to the return cannula flow. These findings underscore the need for optimized cannula placement and ventilatory strategies to minimize hemodynamic instability during advanced neonatal therapy.
中心静脉压(CVP)监测为血流动力学变化提供了有价值的见解;然而,它在接受先进治疗的新生儿缺氧缺血性脑病(HIE)中的应用仍有待探索。本研究旨在评估不同条件下CVP的动态,包括高平均气道压(MAP),新生儿持续性肺动脉高压(PPHN),以及吸入一氧化氮(iNO)和体外膜氧合(ECMO)治疗。方法:本回顾性研究纳入18例诊断为HIE的新生儿,接受脑低温治疗并适当放置脐静脉导管(UVC)监测CVP。分析CVP值与高MAP(≥10 cmH₂O)、PPHN状态以及治疗前和治疗后干预(如iNO和ECMO)的关系。采用Mann-Whitney U检验对连续变量进行统计学比较,显著性设置为p。结果:高MAP组新生儿的平均CVP值显著高于正常MAP组(6 vs 5 mmHg, p = 0.03)。与无PPHN的高MAP组相比,PPHN +高MAP组的平均CVP、氧合指数和FiO₂水平均显著升高。注射iNO显著降低了平均CVP (iNO前7 mmHg vs. iNO后4 mmHg, p = 0.04),而VV-ECMO启动导致CVP升高(ecmo前平均CVP: 8 mmHg vs. ecmo后13 mmHg, p = 0.03)。讨论:通过UVC监测CVP提供了HIE新生儿血流动力学变化的关键信息,特别是在高MAP和PPHN条件下。虽然iNO有效降低了CVP并改善了氧合,但VV-ECMO导致CVP升高,可能是由于回管流量。这些发现强调了优化插管放置和通气策略的必要性,以尽量减少晚期新生儿治疗过程中的血流动力学不稳定。
期刊介绍:
Frontiers in Pediatrics (Impact Factor 2.33) publishes rigorously peer-reviewed research broadly across the field, from basic to clinical research that meets ongoing challenges in pediatric patient care and child health. Field Chief Editors Arjan Te Pas at Leiden University and Michael L. Moritz at the Children''s Hospital of Pittsburgh are supported by an outstanding Editorial Board of international experts. This multidisciplinary open-access journal is at the forefront of disseminating and communicating scientific knowledge and impactful discoveries to researchers, academics, clinicians and the public worldwide.
Frontiers in Pediatrics also features Research Topics, Frontiers special theme-focused issues managed by Guest Associate Editors, addressing important areas in pediatrics. In this fashion, Frontiers serves as an outlet to publish the broadest aspects of pediatrics in both basic and clinical research, including high-quality reviews, case reports, editorials and commentaries related to all aspects of pediatrics.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


