{"title":"Hybrid Thoracoabdominal Aortic Aneurysm Repair After Prior Abdominal Aortic Aneurysm Repair: Safety and Outcomes.","authors":"Kazuhiro Ueno, Takashi Shuto, Takayuki Kawashima, Tomoyuki Wada, Katsuki Oji, Takeaki Dotsu, Norio Hongo, Yoshiki Asayama, Shinji Miyamoto","doi":"10.1093/icvts/ivaf230","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Hybrid repair of thoracoabdominal aortic aneurysms (TAAA), combining visceral debranching and thoracic endovascular aortic repair, is a less invasive alternative to open surgery. However, data on long-term outcomes, especially in patients with prior open abdominal aortic aneurysm (AAA) repair, are limited. This study compares outcomes of hybrid TAAA repair in patients undergoing concomitant AAA repair vs those with prior open AAA repair.</p><p><strong>Methods: </strong>Between January 2007 and January 2024, 132 TAAA repairs were performed at our institution. We retrospectively analysed 80 patients who underwent hybrid TAAA repair. After excluding emergency cases and those without AAA repair, 67 patients were included: 50 with concomitant AAA repair (Group C) and 17 with prior open AAA repair (Group P). Perioperative outcomes, complications, and long-term survival and aortic event-free rates were compared between groups.</p><p><strong>Results: </strong>The median age was 72.0 years (IQR: 65.0-80.8) in Group C and 75.0 years (IQR: 70.0-82.0) in Group P (P = .34). Hospital mortality was 3.0% overall, with no significant group differences. Mean follow-up was 5.0 ± 3.1 years. Five-year overall survival was 69% in Group C and 63% in Group P (P = .22). Freedom from aortic events at 5 years was 92% in Group C and 83% in Group P (P = .19). IPTW-adjusted analyses confirmed no significant differences between the groups.</p><p><strong>Conclusions: </strong>Hybrid TAAA repair can be safely performed for patients with prior AAA open repair, with acceptable long-term outcomes after appropriate patient selection.</p>","PeriodicalId":73406,"journal":{"name":"Interdisciplinary cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-10-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12512131/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interdisciplinary cardiovascular and thoracic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/icvts/ivaf230","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Hybrid repair of thoracoabdominal aortic aneurysms (TAAA), combining visceral debranching and thoracic endovascular aortic repair, is a less invasive alternative to open surgery. However, data on long-term outcomes, especially in patients with prior open abdominal aortic aneurysm (AAA) repair, are limited. This study compares outcomes of hybrid TAAA repair in patients undergoing concomitant AAA repair vs those with prior open AAA repair.
Methods: Between January 2007 and January 2024, 132 TAAA repairs were performed at our institution. We retrospectively analysed 80 patients who underwent hybrid TAAA repair. After excluding emergency cases and those without AAA repair, 67 patients were included: 50 with concomitant AAA repair (Group C) and 17 with prior open AAA repair (Group P). Perioperative outcomes, complications, and long-term survival and aortic event-free rates were compared between groups.
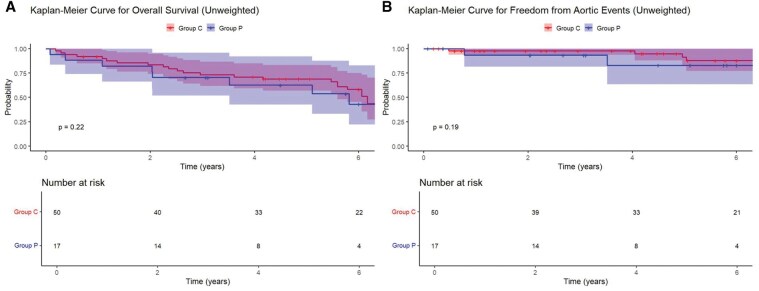
Results: The median age was 72.0 years (IQR: 65.0-80.8) in Group C and 75.0 years (IQR: 70.0-82.0) in Group P (P = .34). Hospital mortality was 3.0% overall, with no significant group differences. Mean follow-up was 5.0 ± 3.1 years. Five-year overall survival was 69% in Group C and 63% in Group P (P = .22). Freedom from aortic events at 5 years was 92% in Group C and 83% in Group P (P = .19). IPTW-adjusted analyses confirmed no significant differences between the groups.
Conclusions: Hybrid TAAA repair can be safely performed for patients with prior AAA open repair, with acceptable long-term outcomes after appropriate patient selection.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


