Video-Assisted Thoracoscopic Surgery Versus Tube Thoracostomy with Fibrinolytics for Treatment of Empyema in Children: A Meta-Analysis of Randomized Controlled Studies.
Maria Enrica Miscia, Giuseppe Lauriti, Dacia Di Renzo, Valentina Cascini, Gabriele Lisi
{"title":"Video-Assisted Thoracoscopic Surgery Versus Tube Thoracostomy with Fibrinolytics for Treatment of Empyema in Children: A Meta-Analysis of Randomized Controlled Studies.","authors":"Maria Enrica Miscia, Giuseppe Lauriti, Dacia Di Renzo, Valentina Cascini, Gabriele Lisi","doi":"10.3390/children12091225","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b>: The British Thoracic Society recommended tube thoracostomy plus intra-pleural fibrinolytics to treat empyema in children in 2005. However, numerous comparative studies have suggested Video-Assisted Thoracoscopic Surgery (VATS) as a first line of treatment for pediatric empyema due to its superior outcomes, including shorter length of hospital stay (LOS). This meta-analysis aimed to compare the following: (1) the LOS for VATS versus fibrinolytics to treat empyema in children; (2) secondary post-operative outcomes (fever, O<sub>2</sub> support, time taken for chest tube removal, analgesia, complications, failure, and abnormal chest X-ray at follow-up). <b>Methods</b>: The study was conducted according to PRISMA guidelines. A systematic search of PubMed, Cochrane, Web of Science, and Scopus was conducted according to PRISMA guidelines. Two independent investigators identified relevant studies, excluding case reports, opinion articles, and gray literature publications. A meta-analysis of randomized controlled trials (RCTs) was performed using RevMan 5.4, with data expressed as mean ± standard deviation (SD). <b>Results</b>: Of 1374 abstracts screened, 104 full-text articles were analyzed, and 6 RCTs (345 patients) were included in the meta-analysis. Patients undergoing VATS had significantly shorter LOS compared to those receiving fibrinolytics (9.1 ± 1.8 vs. 11.5 ± 2.5 days, <i>p</i> = 0.05). VATS patients also experienced shorter postoperative fever duration (4.2 ± 0.8 vs. 6.9 ± 4.6 days, <i>p</i> = 0.007) and earlier chest tube removal (5.0 ± 2.6 vs. 9.5 ± 3.3 days, <i>p</i> = 0.01). No significant differences were found between the two groups for other secondary outcomes. <b>Conclusions</b>: Children with empyema appear to benefit from VATS compared to tube thoracostomy plus fibrinolytics, with improved outcomes. Further RCTs are needed to corroborate these results.</p>","PeriodicalId":48588,"journal":{"name":"Children-Basel","volume":"12 9","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2025-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12468689/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Children-Basel","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/children12091225","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
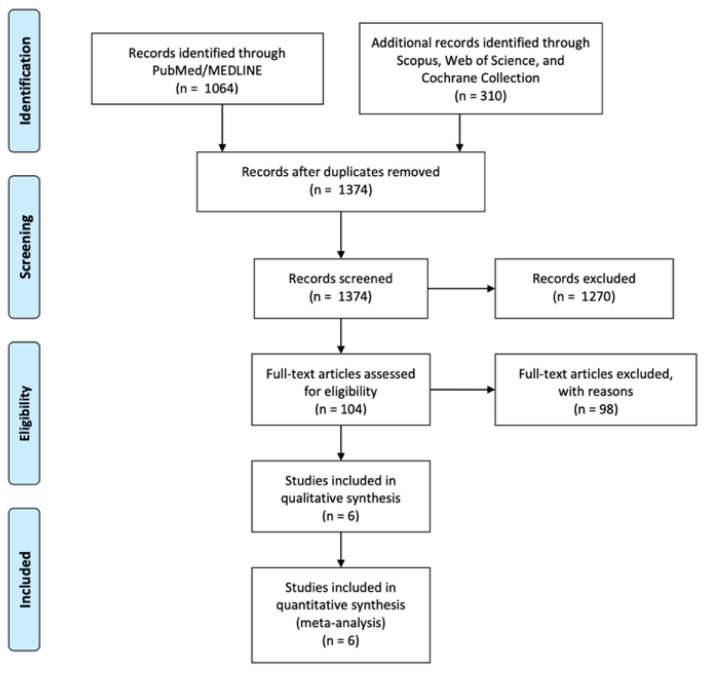
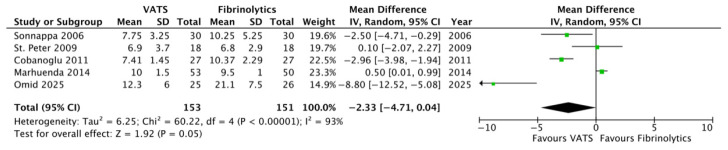
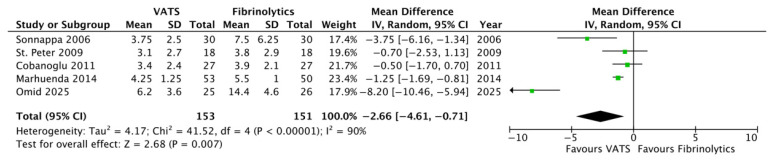
Background: The British Thoracic Society recommended tube thoracostomy plus intra-pleural fibrinolytics to treat empyema in children in 2005. However, numerous comparative studies have suggested Video-Assisted Thoracoscopic Surgery (VATS) as a first line of treatment for pediatric empyema due to its superior outcomes, including shorter length of hospital stay (LOS). This meta-analysis aimed to compare the following: (1) the LOS for VATS versus fibrinolytics to treat empyema in children; (2) secondary post-operative outcomes (fever, O2 support, time taken for chest tube removal, analgesia, complications, failure, and abnormal chest X-ray at follow-up). Methods: The study was conducted according to PRISMA guidelines. A systematic search of PubMed, Cochrane, Web of Science, and Scopus was conducted according to PRISMA guidelines. Two independent investigators identified relevant studies, excluding case reports, opinion articles, and gray literature publications. A meta-analysis of randomized controlled trials (RCTs) was performed using RevMan 5.4, with data expressed as mean ± standard deviation (SD). Results: Of 1374 abstracts screened, 104 full-text articles were analyzed, and 6 RCTs (345 patients) were included in the meta-analysis. Patients undergoing VATS had significantly shorter LOS compared to those receiving fibrinolytics (9.1 ± 1.8 vs. 11.5 ± 2.5 days, p = 0.05). VATS patients also experienced shorter postoperative fever duration (4.2 ± 0.8 vs. 6.9 ± 4.6 days, p = 0.007) and earlier chest tube removal (5.0 ± 2.6 vs. 9.5 ± 3.3 days, p = 0.01). No significant differences were found between the two groups for other secondary outcomes. Conclusions: Children with empyema appear to benefit from VATS compared to tube thoracostomy plus fibrinolytics, with improved outcomes. Further RCTs are needed to corroborate these results.
背景:2005年,英国胸科学会推荐导管开胸联合胸膜内纤溶药物治疗儿童脓胸。然而,许多比较研究表明,视频辅助胸腔镜手术(VATS)由于其优越的疗效,包括住院时间(LOS)较短,可作为儿童脓胸的一线治疗方法。本荟萃分析旨在比较以下内容:(1)VATS与纤溶药物治疗儿童脓胸的LOS;(2)术后继发结果(发热、氧支持、拔胸管时间、镇痛、并发症、衰竭、随访时胸片异常)。方法:按照PRISMA指南进行研究。根据PRISMA指南系统检索PubMed、Cochrane、Web of Science和Scopus。两名独立调查人员确定了相关研究,排除了病例报告、观点文章和灰色文献出版物。采用RevMan 5.4对随机对照试验(RCTs)进行meta分析,数据以均数±标准差(SD)表示。结果:在筛选的1374篇摘要中,分析了104篇全文文章,并将6项rct(345例患者)纳入meta分析。与接受纤溶药物治疗的患者相比,接受VATS治疗的患者LOS明显缩短(9.1±1.8天vs 11.5±2.5天,p = 0.05)。VATS患者术后发热时间较短(4.2±0.8 vs. 6.9±4.6 d, p = 0.007),胸管拔除时间较早(5.0±2.6 vs. 9.5±3.3 d, p = 0.01)。两组间其他次要结果无显著差异。结论:与管式开胸术加纤溶剂治疗相比,VATS治疗有明显的效果。需要进一步的随机对照试验来证实这些结果。
期刊介绍:
Children is an international, open access journal dedicated to a streamlined, yet scientifically rigorous, dissemination of peer-reviewed science related to childhood health and disease in developed and developing countries.
The publication focuses on sharing clinical, epidemiological and translational science relevant to children’s health. Moreover, the primary goals of the publication are to highlight under‑represented pediatric disciplines, to emphasize interdisciplinary research and to disseminate advances in knowledge in global child health. In addition to original research, the journal publishes expert editorials and commentaries, clinical case reports, and insightful communications reflecting the latest developments in pediatric medicine. By publishing meritorious articles as soon as the editorial review process is completed, rather than at predefined intervals, Children also permits rapid open access sharing of new information, allowing us to reach the broadest audience in the most expedient fashion.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


