Tumour-Infiltrating Lymphocytes, Tumour Cell Density, and Response to Neoadjuvant Short-Course Radiotherapy in Rectal Cancer: A Translational Sub-Study from the MRC CR07 Clinical Trial.
Jonathan P Callaghan, Ross Jarrett, Alice C Westwood, Jon Laye, Philip Quirke, Derek R Magee, Daniel Bottomley, David Sebag-Montefiore, Lindsay Thompson, Angela Meade, Heike I Grabsch, Nicholas P West
{"title":"Tumour-Infiltrating Lymphocytes, Tumour Cell Density, and Response to Neoadjuvant Short-Course Radiotherapy in Rectal Cancer: A Translational Sub-Study from the MRC CR07 Clinical Trial.","authors":"Jonathan P Callaghan, Ross Jarrett, Alice C Westwood, Jon Laye, Philip Quirke, Derek R Magee, Daniel Bottomley, David Sebag-Montefiore, Lindsay Thompson, Angela Meade, Heike I Grabsch, Nicholas P West","doi":"10.3390/cancers17183040","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b>: Rectal cancer is common and frequently treated with neoadjuvant radiotherapy prior to surgery to reduce the risk of tumour recurrence. However, the therapeutic benefits and side effects of radiotherapy can vary between patients, and there are currently no validated biomarkers to predict treatment response. Tumour cell density (TCD) and tumour-infiltrating lymphocyte (TIL) density are proven prognostic biomarkers in colorectal cancer; however, their utility in predicting radiotherapy response remains unclear. We assessed the prognostic and predictive value of TCD and TIL density in rectal cancer patients treated with radiotherapy. <b>Methods</b>: TCD was quantified using a manual point-counting method in 253 pre-treatment biopsies and across the entire tumour area of 569 resection specimens from the MRC CR07 clinical trial, which randomised patients to either neoadjuvant short-course radiotherapy (SCRT) or straight to surgery (control). TIL density was measured in 102 biopsies and matched resection specimens (73 SCRT, 29 control) across different tumour areas using deep learning-based cell detection in MIM (HeteroGenius Ltd., Leeds, UK). Cutoffs for low/high-TCD and TIL density were both pre-defined and derived from survival data using the survminer R package. Survival analyses were performed to evaluate the predictive and prognostic value of TCD/TIL in relation to overall and cancer-specific survival. <b>Results</b>: TCD in the resection specimens was lower in the SCRT group (19.9%, IQR 12.9-26.7%) than the control group (34.3%, IQR 27.7-40.5%, <i>p</i> < 0.001). In control resections, low-TCD was associated with a higher risk of all-cause mortality (HR 2.20, 95% CI 1.41-3.44, <i>p</i> < 0.001) and cancer-related death (HR 2.69, 95% CI 1.41-5.13, <i>p</i> = 0.0026). In contrast, after SCRT, low resection TCD was associated with a reduced risk of death (HR 0.63, 95% CI 0.40-0.98, <i>p</i> = 0.04). In the SCRT group, low biopsy TCD prior to radiotherapy was associated with a reduced risk of cancer-related death (HR 0.34, 95% CI 0.13-0.89, <i>p</i> = 0.028). Across both trial arms, TIL density was higher in pre-treatment biopsies than resections (2492 vs. 1304/mm<sup>2</sup>, <i>p</i> < 0.001). Low biopsy TIL density was associated with an increased risk of all-cause mortality (HR 2.43, 95% CI 1.24-4.76, <i>p</i> = 0.01). The SCRT group had lower TIL density in the resection compared with controls (1210 vs. 1615/mm<sup>2</sup>, <i>p</i> < 0.001), and low resection TIL density across the whole tumour area was associated with a higher risk of death (HR 2.55, 95% CI 1.11-5.87, <i>p</i> = 0.027). <b>Conclusions</b>: Our findings support the role of TCD and TIL density as quantitative biomarkers in rectal cancer patients. TCD can be used to assess the degree of response to radiotherapy, and contrasting survival associations are observed between straight-to-surgery and SCRT-treated patients. This study raises the possibility of using TCD as both a prognostic and predictive biomarker. TIL density failed to show predictive value but demonstrated expected prognostic associations.</p>","PeriodicalId":9681,"journal":{"name":"Cancers","volume":"17 18","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2025-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12468021/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancers","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/cancers17183040","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
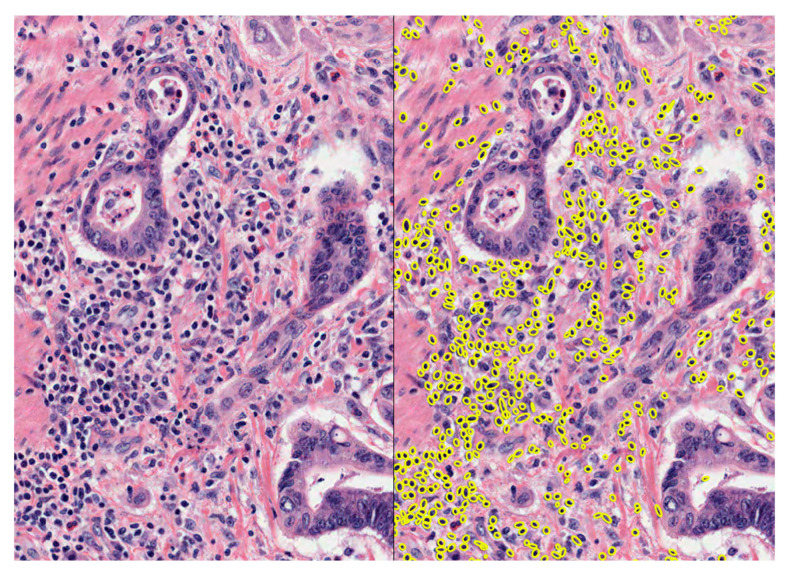
Background: Rectal cancer is common and frequently treated with neoadjuvant radiotherapy prior to surgery to reduce the risk of tumour recurrence. However, the therapeutic benefits and side effects of radiotherapy can vary between patients, and there are currently no validated biomarkers to predict treatment response. Tumour cell density (TCD) and tumour-infiltrating lymphocyte (TIL) density are proven prognostic biomarkers in colorectal cancer; however, their utility in predicting radiotherapy response remains unclear. We assessed the prognostic and predictive value of TCD and TIL density in rectal cancer patients treated with radiotherapy. Methods: TCD was quantified using a manual point-counting method in 253 pre-treatment biopsies and across the entire tumour area of 569 resection specimens from the MRC CR07 clinical trial, which randomised patients to either neoadjuvant short-course radiotherapy (SCRT) or straight to surgery (control). TIL density was measured in 102 biopsies and matched resection specimens (73 SCRT, 29 control) across different tumour areas using deep learning-based cell detection in MIM (HeteroGenius Ltd., Leeds, UK). Cutoffs for low/high-TCD and TIL density were both pre-defined and derived from survival data using the survminer R package. Survival analyses were performed to evaluate the predictive and prognostic value of TCD/TIL in relation to overall and cancer-specific survival. Results: TCD in the resection specimens was lower in the SCRT group (19.9%, IQR 12.9-26.7%) than the control group (34.3%, IQR 27.7-40.5%, p < 0.001). In control resections, low-TCD was associated with a higher risk of all-cause mortality (HR 2.20, 95% CI 1.41-3.44, p < 0.001) and cancer-related death (HR 2.69, 95% CI 1.41-5.13, p = 0.0026). In contrast, after SCRT, low resection TCD was associated with a reduced risk of death (HR 0.63, 95% CI 0.40-0.98, p = 0.04). In the SCRT group, low biopsy TCD prior to radiotherapy was associated with a reduced risk of cancer-related death (HR 0.34, 95% CI 0.13-0.89, p = 0.028). Across both trial arms, TIL density was higher in pre-treatment biopsies than resections (2492 vs. 1304/mm2, p < 0.001). Low biopsy TIL density was associated with an increased risk of all-cause mortality (HR 2.43, 95% CI 1.24-4.76, p = 0.01). The SCRT group had lower TIL density in the resection compared with controls (1210 vs. 1615/mm2, p < 0.001), and low resection TIL density across the whole tumour area was associated with a higher risk of death (HR 2.55, 95% CI 1.11-5.87, p = 0.027). Conclusions: Our findings support the role of TCD and TIL density as quantitative biomarkers in rectal cancer patients. TCD can be used to assess the degree of response to radiotherapy, and contrasting survival associations are observed between straight-to-surgery and SCRT-treated patients. This study raises the possibility of using TCD as both a prognostic and predictive biomarker. TIL density failed to show predictive value but demonstrated expected prognostic associations.
背景:直肠癌是一种常见病,术前常进行新辅助放疗以降低肿瘤复发的风险。然而,放疗的治疗益处和副作用可能因患者而异,目前还没有经过验证的生物标志物来预测治疗反应。肿瘤细胞密度(TCD)和肿瘤浸润淋巴细胞密度(TIL)是结直肠癌预后的生物标志物;然而,它们在预测放疗反应方面的效用尚不清楚。我们评估了TCD和TIL密度对直肠癌放疗患者的预后和预测价值。方法:在MRC CR07临床试验的253个治疗前活检和569个切除标本的整个肿瘤区域中,使用手动点计数法对TCD进行量化,该试验将患者随机分配到新辅助短期放疗(SCRT)或直接手术(对照组)。在MIM (HeteroGenius Ltd, Leeds, UK)中使用基于深度学习的细胞检测技术测量了102例活检和匹配的切除标本(73例SCRT, 29例对照)不同肿瘤区域的TIL密度。低/高tcd和TIL密度的截止值都是预先定义的,并使用survminer R包从生存数据中导出。进行生存分析,以评估TCD/TIL在总体和癌症特异性生存方面的预测和预后价值。结果:SCRT组切除标本TCD (19.9%, IQR 12.9 ~ 26.7%)低于对照组(34.3%,IQR 27.7 ~ 40.5%, p < 0.001)。在对照切除中,低tcd与全因死亡率(HR 2.20, 95% CI 1.41-3.44, p < 0.001)和癌症相关死亡(HR 2.69, 95% CI 1.41-5.13, p = 0.0026)的风险较高相关。相比之下,在SCRT后,低切除TCD与死亡风险降低相关(HR 0.63, 95% CI 0.40-0.98, p = 0.04)。在SCRT组中,放疗前低活检TCD与癌症相关死亡风险降低相关(HR 0.34, 95% CI 0.13-0.89, p = 0.028)。在两个试验组中,治疗前活检的TIL密度高于切除(2492比1304/mm2, p < 0.001)。低活检TIL密度与全因死亡风险增加相关(HR 2.43, 95% CI 1.24-4.76, p = 0.01)。与对照组相比,SCRT组在切除时TIL密度较低(1210比1615/mm2, p < 0.001),整个肿瘤区域的低切除TIL密度与较高的死亡风险相关(HR 2.55, 95% CI 1.11-5.87, p = 0.027)。结论:我们的研究结果支持TCD和TIL密度作为直肠癌患者定量生物标志物的作用。TCD可用于评估对放疗的反应程度,在直接手术和scrt治疗的患者之间观察到截然不同的生存关联。这项研究提出了使用TCD作为预后和预测性生物标志物的可能性。TIL密度没有显示出预测价值,但显示出预期的预后关联。
期刊介绍:
Cancers (ISSN 2072-6694) is an international, peer-reviewed open access journal on oncology. It publishes reviews, regular research papers and short communications. Our aim is to encourage scientists to publish their experimental and theoretical results in as much detail as possible. There is no restriction on the length of the papers. The full experimental details must be provided so that the results can be reproduced.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


