Ahmed Alnajar, Amber Collier, Mehmet Akcin, John I Lew, Tanaz M Vaghaiwalla
{"title":"Centralized Surgical Care Improves Survival in Non-Functional Well-Differentiated Pancreatic Neuroendocrine Tumors.","authors":"Ahmed Alnajar, Amber Collier, Mehmet Akcin, John I Lew, Tanaz M Vaghaiwalla","doi":"10.3390/cancers17183030","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Non-functional well-differentiated pancreatic neuroendocrine tumors (WD-PanNETs) are complex, heterogeneous malignancies with variable prognosis. Despite guideline recommendations, disparities in access to specialized care may impact survival. This study examines whether treatment facility type, geographic travel distance, and treatment modalities are associated with survival outcomes in patients diagnosed with WD-PanNETs. <b>Results:</b> Among 20,174 patients with WD-PanNETs, the median age was 62 years (IQR: 52-70), and 54% were men. The majority were treated at non-academic hospitals (76%), with 2.9% traveling >250 miles for care. Patients treated at non-academic hospitals (24%) had 50% lower 15-year survival rates compared to those treated at academic hospitals (58%) and integrated hospitals (56%) (<i>p</i> < 0.001). Patients traveling >250 miles had a 72% 15-year survival rate, compared to 43% for those traveling <12.5 miles (<i>p</i> < 0.001). In the context of facility-type and geographic distance, treatment at non-academic hospitals <250 miles was associated with a 21% higher mortality risk (HR 1.21, 95% CI 1.12-1.31, <i>p</i> < 0.001), and treatment at low-volume hospitals increased mortality risk by 25% (HR 1.25, 95% CI 1.14-1.37, <i>p</i> < 0.001). In contrast, primary tumor resection was associated with a 64% reduction in mortality risk (HR 0.36, 95% CI 0.33-0.38, <i>p</i> < 0.001), which remained significant at all disease stages. <b>Conclusion:</b> Treatment at academic or high-volume centers and longer travel distances were associated with improved OS in patients with WD-PanNETs. Primary tumor resection remains critical, while systemic therapies were primarily used in later-stage disease. These findings support policies that improve access to centralized, multidisciplinary care.</p>","PeriodicalId":9681,"journal":{"name":"Cancers","volume":"17 18","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2025-09-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12468637/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancers","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/cancers17183030","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
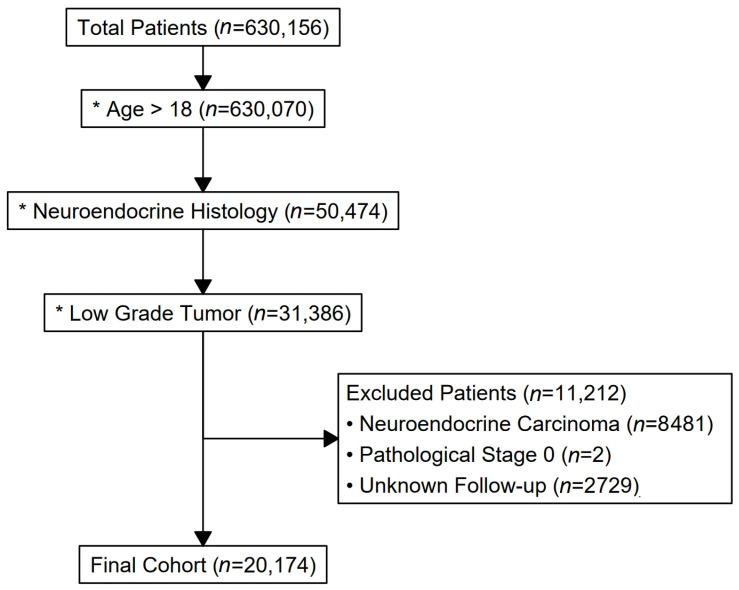
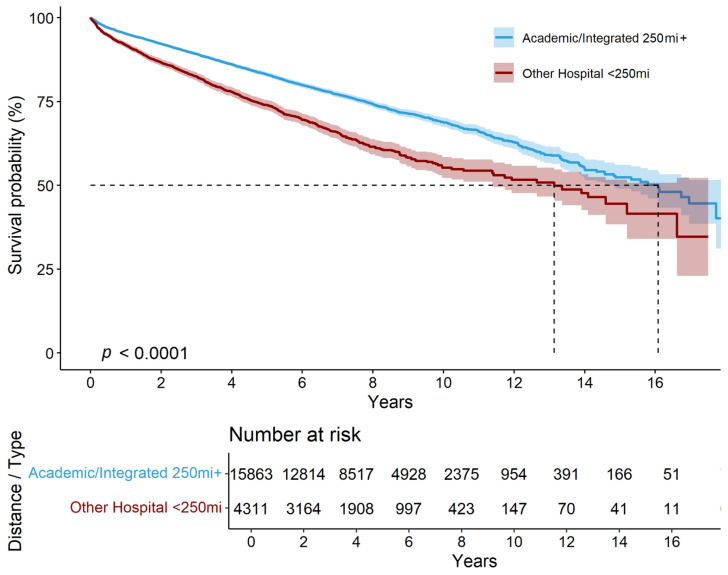
Background: Non-functional well-differentiated pancreatic neuroendocrine tumors (WD-PanNETs) are complex, heterogeneous malignancies with variable prognosis. Despite guideline recommendations, disparities in access to specialized care may impact survival. This study examines whether treatment facility type, geographic travel distance, and treatment modalities are associated with survival outcomes in patients diagnosed with WD-PanNETs. Results: Among 20,174 patients with WD-PanNETs, the median age was 62 years (IQR: 52-70), and 54% were men. The majority were treated at non-academic hospitals (76%), with 2.9% traveling >250 miles for care. Patients treated at non-academic hospitals (24%) had 50% lower 15-year survival rates compared to those treated at academic hospitals (58%) and integrated hospitals (56%) (p < 0.001). Patients traveling >250 miles had a 72% 15-year survival rate, compared to 43% for those traveling <12.5 miles (p < 0.001). In the context of facility-type and geographic distance, treatment at non-academic hospitals <250 miles was associated with a 21% higher mortality risk (HR 1.21, 95% CI 1.12-1.31, p < 0.001), and treatment at low-volume hospitals increased mortality risk by 25% (HR 1.25, 95% CI 1.14-1.37, p < 0.001). In contrast, primary tumor resection was associated with a 64% reduction in mortality risk (HR 0.36, 95% CI 0.33-0.38, p < 0.001), which remained significant at all disease stages. Conclusion: Treatment at academic or high-volume centers and longer travel distances were associated with improved OS in patients with WD-PanNETs. Primary tumor resection remains critical, while systemic therapies were primarily used in later-stage disease. These findings support policies that improve access to centralized, multidisciplinary care.
期刊介绍:
Cancers (ISSN 2072-6694) is an international, peer-reviewed open access journal on oncology. It publishes reviews, regular research papers and short communications. Our aim is to encourage scientists to publish their experimental and theoretical results in as much detail as possible. There is no restriction on the length of the papers. The full experimental details must be provided so that the results can be reproduced.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


