Ci-Wen Luo, Meng-Hao Chang, Lan Lin, Frank Cheau-Feng Lin, Shih-Wei Chen, Yu-Hsiang Kuan, Pei-Chi Tsai, Ji-Kuen Yu, Stella Chin-Shaw Tsai
{"title":"Long-Term Survival After Thyroidectomy for Thyroid Cancer: A Propensity-Matched TriNetX Study with Specialty-Stratified Analyses.","authors":"Ci-Wen Luo, Meng-Hao Chang, Lan Lin, Frank Cheau-Feng Lin, Shih-Wei Chen, Yu-Hsiang Kuan, Pei-Chi Tsai, Ji-Kuen Yu, Stella Chin-Shaw Tsai","doi":"10.3390/cancers17183051","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/objectives: </strong>Whether thyroidectomy confers a long-term survival advantage over non-surgical management in real-world practice remains uncertain. We primarily evaluated the association between surgery and all-cause mortality in thyroid cancer; specialty-stratified outcomes were prespecified as secondary, exploratory analyses.</p><p><strong>Methods: </strong>Using the TriNetX US Collaborative Network (2008-2024), we identified adults with thyroid cancer and created 1:1 propensity score-matched cohorts of patients who did or did not undergo thyroidectomy, balancing demographics, comorbidities, medications, and laboratory variables. Overall survival was assessed with Kaplan-Meier curves and Cox proportional hazard models. Among the surgical patients, we performed exploratory analyses stratified by operating specialty (otolaryngology-head and neck surgery (reference) vs. general/endocrine surgery and other/unknown, reported descriptively).</p><p><strong>Results: </strong>After matching, 49,219 patients were included per cohort. Thyroidectomy was associated with lower long-term mortality versus non-surgical care (adjusted HR 0.685, 95% CI 0.652-0.721). Among the surgical patients, secondary, exploratory specialty-stratified analyses suggested differences: compared with otolaryngology-head and neck surgery (ENT-HNS; reference), general/endocrine surgery (GS/ES) had a lower adjusted hazard of death (aHR 0.561, 95% CI 0.481-0.654), whereas other/unknown specialties had a higher adjusted hazard (aHR 1.583, 95% CI 1.302-1.924). These patterns are hypothesis-generating and may reflect residual confounding, including the tumor stage and histology, referral pathways, and surgeon or center experience.</p><p><strong>Conclusions: </strong>In a large, propensity-matched real-world cohort, surgery was linked to improved long-term survival regarding thyroid cancer. Observed specialty-related variation should be interpreted cautiously, and prospective studies incorporating tumor-level variables and provider/center characteristics are needed. Emphasis should remain on timely surgery within multidisciplinary care pathways.</p>","PeriodicalId":9681,"journal":{"name":"Cancers","volume":"17 18","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2025-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12468916/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancers","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/cancers17183051","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background/objectives: Whether thyroidectomy confers a long-term survival advantage over non-surgical management in real-world practice remains uncertain. We primarily evaluated the association between surgery and all-cause mortality in thyroid cancer; specialty-stratified outcomes were prespecified as secondary, exploratory analyses.
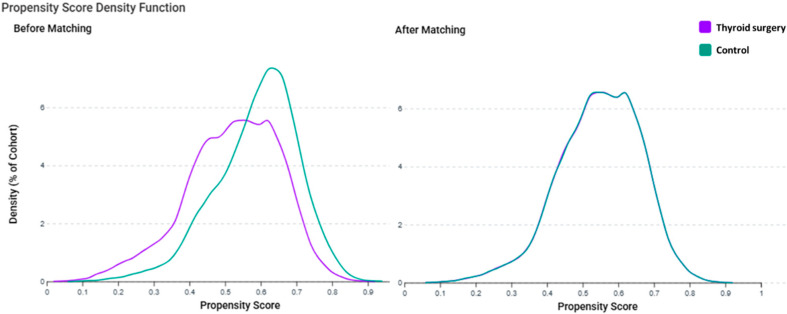
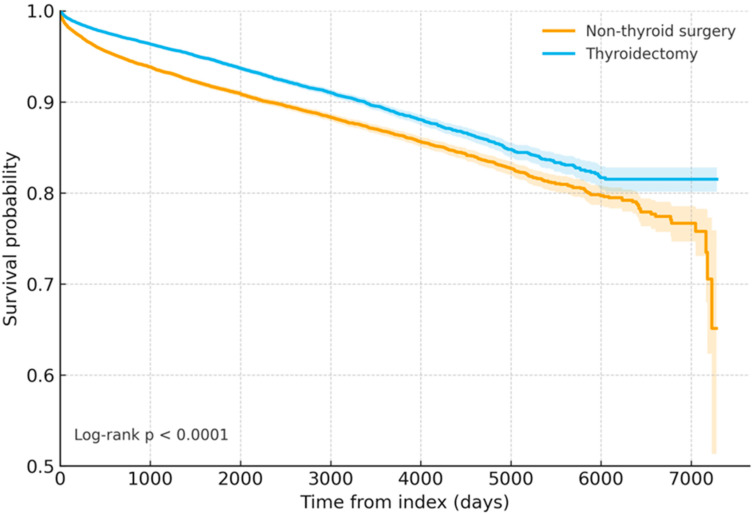
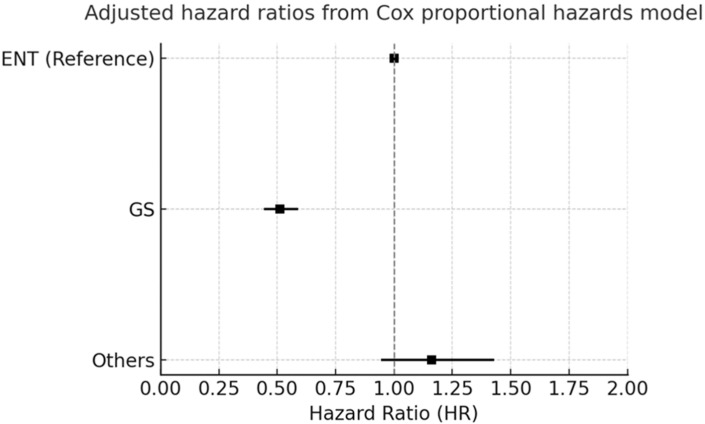
Methods: Using the TriNetX US Collaborative Network (2008-2024), we identified adults with thyroid cancer and created 1:1 propensity score-matched cohorts of patients who did or did not undergo thyroidectomy, balancing demographics, comorbidities, medications, and laboratory variables. Overall survival was assessed with Kaplan-Meier curves and Cox proportional hazard models. Among the surgical patients, we performed exploratory analyses stratified by operating specialty (otolaryngology-head and neck surgery (reference) vs. general/endocrine surgery and other/unknown, reported descriptively).
Results: After matching, 49,219 patients were included per cohort. Thyroidectomy was associated with lower long-term mortality versus non-surgical care (adjusted HR 0.685, 95% CI 0.652-0.721). Among the surgical patients, secondary, exploratory specialty-stratified analyses suggested differences: compared with otolaryngology-head and neck surgery (ENT-HNS; reference), general/endocrine surgery (GS/ES) had a lower adjusted hazard of death (aHR 0.561, 95% CI 0.481-0.654), whereas other/unknown specialties had a higher adjusted hazard (aHR 1.583, 95% CI 1.302-1.924). These patterns are hypothesis-generating and may reflect residual confounding, including the tumor stage and histology, referral pathways, and surgeon or center experience.
Conclusions: In a large, propensity-matched real-world cohort, surgery was linked to improved long-term survival regarding thyroid cancer. Observed specialty-related variation should be interpreted cautiously, and prospective studies incorporating tumor-level variables and provider/center characteristics are needed. Emphasis should remain on timely surgery within multidisciplinary care pathways.
期刊介绍:
Cancers (ISSN 2072-6694) is an international, peer-reviewed open access journal on oncology. It publishes reviews, regular research papers and short communications. Our aim is to encourage scientists to publish their experimental and theoretical results in as much detail as possible. There is no restriction on the length of the papers. The full experimental details must be provided so that the results can be reproduced.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


