When Right Isn’t Right: Left Femoral Access for EVOQUE Transcatheter Tricuspid Valve Replacement System
IF 2.8
Q3 CARDIAC & CARDIOVASCULAR SYSTEMS
引用次数: 0
Abstract
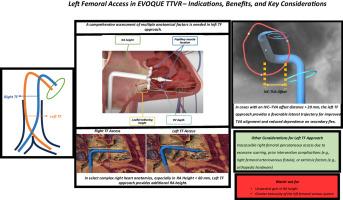
As transcatheter tricuspid valve replacement with the EVOQUE system gains wider clinical adoption, growing experience has highlighted key anatomical considerations that influence procedural success. While right transfemoral (TF) access is the standard approach, it can be technically challenging in patients with complex right heart anatomy, such as low right atrium (RA) height or a large inferior vena cava–tricuspid valve annulus (IVC-TVA) offset. These factors may lead to suboptimal trajectory, impaired coaxiality, and difficult valve deployment. Left TF access offers a potential alternative by providing additional RA height and a more favorable lateral trajectory, allowing improved alignment with the tricuspid valve annulus (TVA). This approach is particularly useful in patients with large short-axis (SAX) offsets (>20 mm) or steep long-axis angles where right TF access may not achieve perpendicular orientation despite secondary catheter flexion. Using a preprocedural cardiac computed tomography angiography (CCTA) scan, anatomical factors such as RAH, leaflet tethering height, RV depth, and papillary muscle location can be evaluated to guide access planning. While left TF access introduces its own technical considerations, including venous tortuosity, excessive unwanted RA height, and increased need for primary flex, it may expand procedural feasibility in anatomically challenging cases. This review outlines real-world scenarios where left-sided access was favored, supporting its use as a safe and effective strategy in selected patients. Further studies are warranted to assess long-term outcomes and to inform the design of next-generation delivery systems capable of accommodating broader anatomical variation.
当右不正确:左股通道经EVOQUE三尖瓣置换术系统
随着EVOQUE系统经导管三尖瓣置换术的临床应用越来越广泛,越来越多的经验强调了影响手术成功的关键解剖学因素。虽然右经股(TF)入路是标准入路,但对于右心脏解剖结构复杂的患者,如右心房(RA)高度低或下腔静脉-三尖瓣环(IVC-TVA)偏移较大,在技术上可能具有挑战性。这些因素可能会导致井眼轨迹不理想、同轴度受损以及阀门部署困难。左侧TF通道提供了一个潜在的替代方案,提供了额外的RA高度和更有利的横向轨迹,可以改善与三尖瓣环(TVA)的对齐。这种方法特别适用于短轴(SAX)偏移量大(> 20mm)或长轴角度陡的患者,尽管二次导管屈曲,但右侧TF通路可能无法实现垂直定向。通过术前心脏计算机断层血管造影(CCTA)扫描,可以评估RAH、小叶栓系高度、右心室深度和乳头肌位置等解剖学因素,以指导通路规划。虽然左侧TF通道引入了自身的技术考虑,包括静脉弯曲,多余的RA高度过高,以及对初级弯曲的需求增加,但它可能会扩大解剖学上具有挑战性的病例的手术可行性。这篇综述概述了现实世界中左侧通路被青睐的情况,支持其作为一种安全有效的策略在选定的患者中使用。需要进一步的研究来评估长期结果,并为设计能够适应更广泛解剖变异的下一代给药系统提供信息。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Structural Heart
Medicine-Cardiology and Cardiovascular Medicine
CiteScore
1.60
自引率
0.00%
发文量
81
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


