The submission title: management of retroperitoneal perforated descending duodenal diverticulum using de pezzer catheter drainage combined with nutritional jejunostomy: a case report and review of the literature.
{"title":"The submission title: management of retroperitoneal perforated descending duodenal diverticulum using de pezzer catheter drainage combined with nutritional jejunostomy: a case report and review of the literature.","authors":"Limin Guo, Shuk Ying Wong, Dongdong Zhang, Lei Guo, Simin Chen, Peng Guo","doi":"10.1186/s12893-025-03163-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Duodenal diverticulum (DD) ranks as the second most prevalent form of intestinal diverticulum and is typically asymptomatic. However, perforations of DD, while rare, are associated with potentially fatal outcomes.</p><p><strong>Presentation of case: </strong>A 78-year-old Chinese male patient presented with epigastric pain after overeating the day before admission. A contrast-enhanced computed tomography (CT) of the abdomen revealed cystic areas of extraluminal air in the posterior periduodenal area. We operated on the patient. A De Pezzer catheter and a nasogastric tube were placed in the duodenal cavity, supplemented by two external drainage tubes. Early postoperative enteral nutrition was facilitated through a jejunal feeding tube. The patient underwent successful surgical intervention and was discharged on the 12th post-operative day without any complications.</p><p><strong>Discussion: </strong>Non-operative management may be suitable for carefully selected patients with stable vital signs and a timely diagnosis. Surgical intervention is necessary if conservative approaches fail or in cases leading to generalized peritonitis or severe sepsis. For posterior DD perforations, it is critical to focus not only on wound repair but also on ensuring adequate drainage and decompression of the periduodenal and intestinal cavities to reduce the risk of fistulas.</p><p><strong>Conclusion: </strong>For patients with perforations of DD, surgical intervention should be advocated, emphasizing on the prevention and treatment of duodenal fistula during the operation. The application of a De Pezzer catheter, nasogastric tube, and additional duodenal drainage, combined with jejunal feeding for nutritional support, adheres to damage control principles and leads to favorable clinical outcomes.</p>","PeriodicalId":49229,"journal":{"name":"BMC Surgery","volume":"25 1","pages":"414"},"PeriodicalIF":1.8000,"publicationDate":"2025-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12465761/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12893-025-03163-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Duodenal diverticulum (DD) ranks as the second most prevalent form of intestinal diverticulum and is typically asymptomatic. However, perforations of DD, while rare, are associated with potentially fatal outcomes.
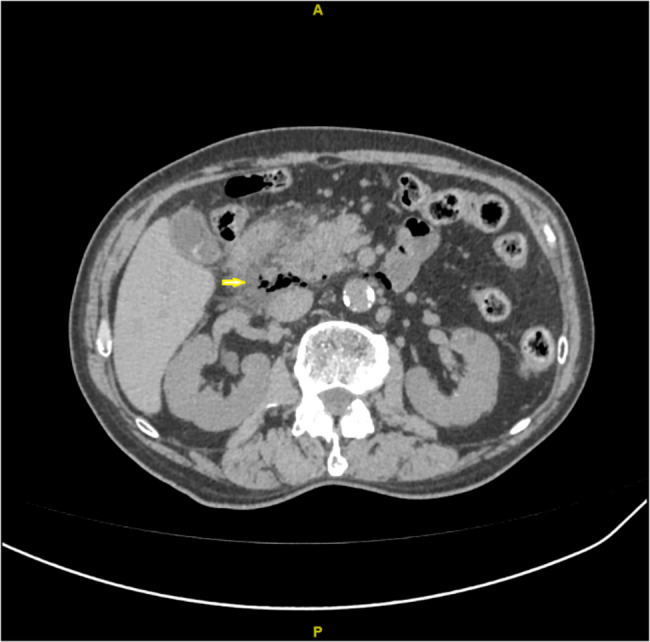
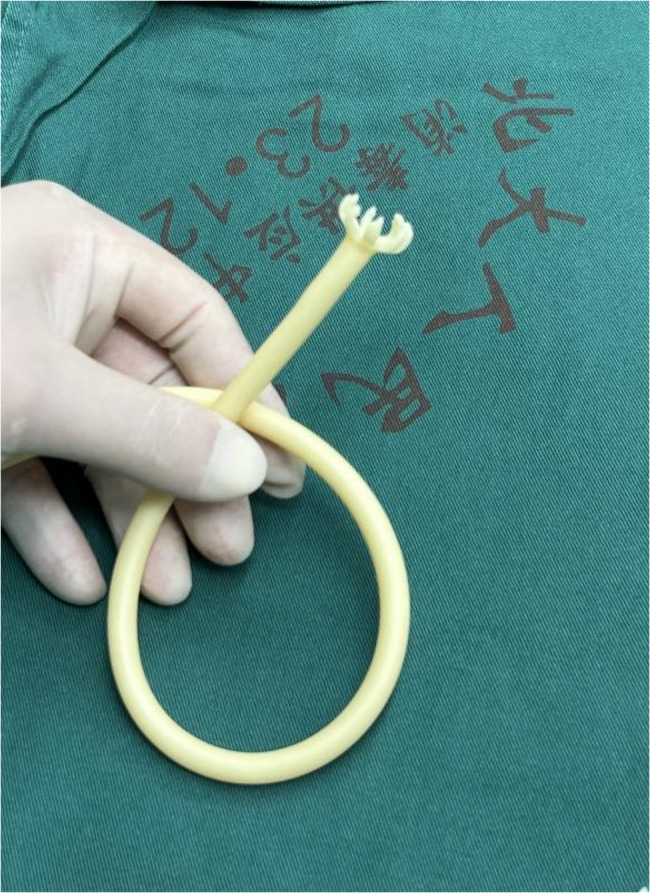
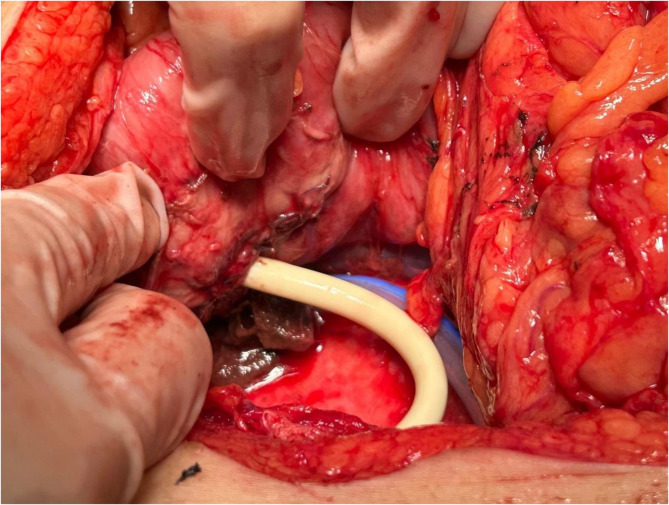
Presentation of case: A 78-year-old Chinese male patient presented with epigastric pain after overeating the day before admission. A contrast-enhanced computed tomography (CT) of the abdomen revealed cystic areas of extraluminal air in the posterior periduodenal area. We operated on the patient. A De Pezzer catheter and a nasogastric tube were placed in the duodenal cavity, supplemented by two external drainage tubes. Early postoperative enteral nutrition was facilitated through a jejunal feeding tube. The patient underwent successful surgical intervention and was discharged on the 12th post-operative day without any complications.
Discussion: Non-operative management may be suitable for carefully selected patients with stable vital signs and a timely diagnosis. Surgical intervention is necessary if conservative approaches fail or in cases leading to generalized peritonitis or severe sepsis. For posterior DD perforations, it is critical to focus not only on wound repair but also on ensuring adequate drainage and decompression of the periduodenal and intestinal cavities to reduce the risk of fistulas.
Conclusion: For patients with perforations of DD, surgical intervention should be advocated, emphasizing on the prevention and treatment of duodenal fistula during the operation. The application of a De Pezzer catheter, nasogastric tube, and additional duodenal drainage, combined with jejunal feeding for nutritional support, adheres to damage control principles and leads to favorable clinical outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


