Intra-hospital MRI transport in neurocritical patients with aneurysmal subarachnoid hemorrhage: complications and clinical impact with predominant continuation of care.
Alexandra Grob, Jonas Georg Buff, Lilian Kriemler, Federica Stretti, Giovanna Brandi
{"title":"Intra-hospital MRI transport in neurocritical patients with aneurysmal subarachnoid hemorrhage: complications and clinical impact with predominant continuation of care.","authors":"Alexandra Grob, Jonas Georg Buff, Lilian Kriemler, Federica Stretti, Giovanna Brandi","doi":"10.1007/s10143-025-03824-3","DOIUrl":null,"url":null,"abstract":"<p><p>Introduction Magnet Resonance Imaging (MRI) is essential for neurocritical care but requires intrahospital transport (IHT) in patients treated in an intensive care unit, which carries significant risks. This study assesses the risk profile and whether the benefits of MRI in aneurysmal subarachnoid hemorrhage (aSAH) outweigh the associated complications of IHT. Method In this retrospective study, all aSAH patients treated in our neurocritical care unit (NCCU) between 2016 and 2023 were screened. Data collection included baseline demographics, hemorrhage severity scores, aneurysm treatment strategies, additional neurosurgical procedures, and need for spasmolysis. IHT- and MRI-related variables were recorded, including timing, indication, duration, and associated physiological parameters such as blood gas values, vital signs, intracranial pressure (ICP), and cerebral perfusion pressure (CPP). The incidence of complications and the clinical impact of MRI findings were evaluated. Statistical comparisons were conducted using the Wilcoxon signed-rank test. Results Of 337 screened patients, 115 (34.1%) patients with aSAH underwent a MRI during the NCCU stay and were included in the analysis, with a total of 156 MRI scans performed. The most common reason for a MRI was ischemia exclusion (61%). Complications occurred in 16% of patients (n = 25), classified as systemic (56%), cerebral (37%), and technical (7%). Blood gas analysis showed no significant changes before and after IHT. In the subgroup of patients with an external ventricular drain (EVD) in situ (n = 93), ICP remained stable, while CPP increased from 85.4 (± 20.5) to 92.1 (± 19.9) mmHg (p = 0.009). Accordingly, systolic BP and MAP increased (p = 0.019 and < 0.001, respectively) and HR decreased by 4/min (p < 0.001). Conclusion We found lower frequency of IHT-related complication in brain MRI after aSAH compared to existing literature reflecting a well-established and safe clinical process. Moreover, MRI findings had a notable impact on key therapeutic decisions, supporting the use of MRI-based IHT in selected cases, provided that a thorough risk-benefit assessment is conducted.</p>","PeriodicalId":19184,"journal":{"name":"Neurosurgical Review","volume":"48 1","pages":"667"},"PeriodicalIF":2.5000,"publicationDate":"2025-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12474663/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurosurgical Review","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10143-025-03824-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
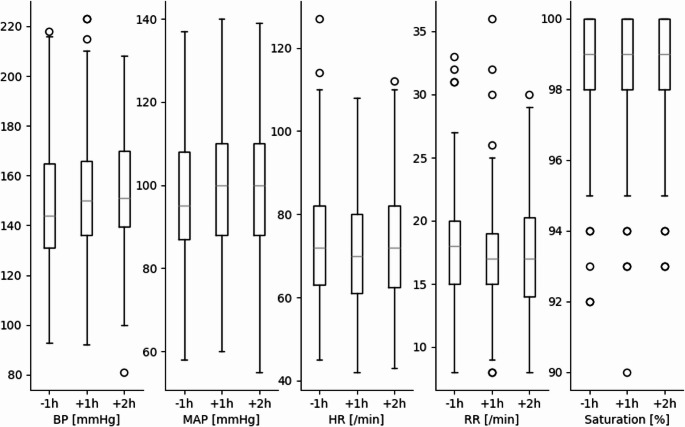
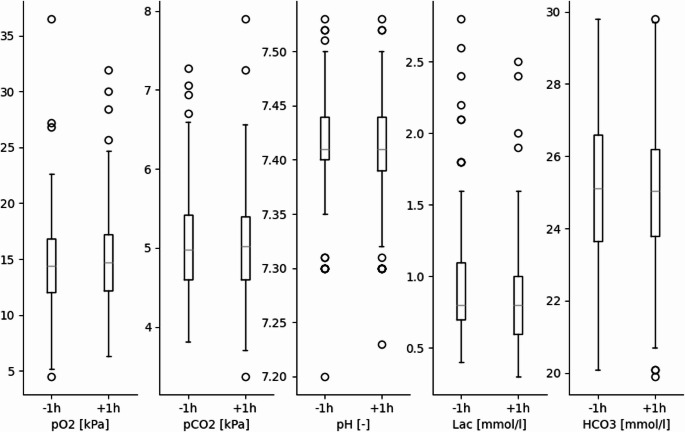
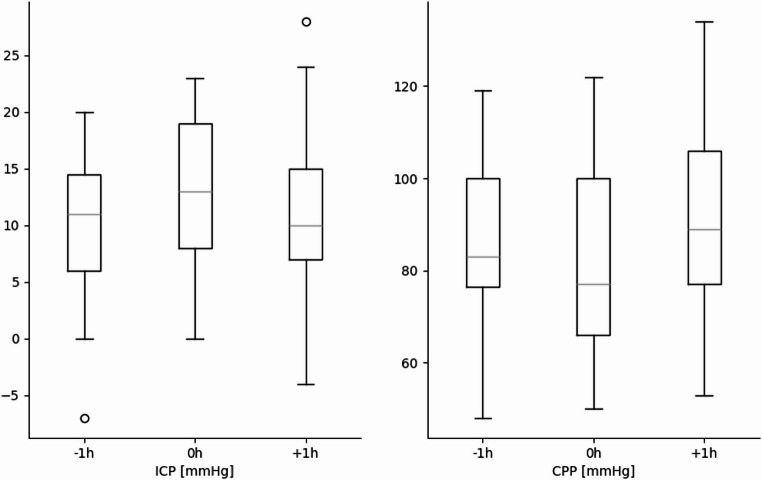
Introduction Magnet Resonance Imaging (MRI) is essential for neurocritical care but requires intrahospital transport (IHT) in patients treated in an intensive care unit, which carries significant risks. This study assesses the risk profile and whether the benefits of MRI in aneurysmal subarachnoid hemorrhage (aSAH) outweigh the associated complications of IHT. Method In this retrospective study, all aSAH patients treated in our neurocritical care unit (NCCU) between 2016 and 2023 were screened. Data collection included baseline demographics, hemorrhage severity scores, aneurysm treatment strategies, additional neurosurgical procedures, and need for spasmolysis. IHT- and MRI-related variables were recorded, including timing, indication, duration, and associated physiological parameters such as blood gas values, vital signs, intracranial pressure (ICP), and cerebral perfusion pressure (CPP). The incidence of complications and the clinical impact of MRI findings were evaluated. Statistical comparisons were conducted using the Wilcoxon signed-rank test. Results Of 337 screened patients, 115 (34.1%) patients with aSAH underwent a MRI during the NCCU stay and were included in the analysis, with a total of 156 MRI scans performed. The most common reason for a MRI was ischemia exclusion (61%). Complications occurred in 16% of patients (n = 25), classified as systemic (56%), cerebral (37%), and technical (7%). Blood gas analysis showed no significant changes before and after IHT. In the subgroup of patients with an external ventricular drain (EVD) in situ (n = 93), ICP remained stable, while CPP increased from 85.4 (± 20.5) to 92.1 (± 19.9) mmHg (p = 0.009). Accordingly, systolic BP and MAP increased (p = 0.019 and < 0.001, respectively) and HR decreased by 4/min (p < 0.001). Conclusion We found lower frequency of IHT-related complication in brain MRI after aSAH compared to existing literature reflecting a well-established and safe clinical process. Moreover, MRI findings had a notable impact on key therapeutic decisions, supporting the use of MRI-based IHT in selected cases, provided that a thorough risk-benefit assessment is conducted.
期刊介绍:
The goal of Neurosurgical Review is to provide a forum for comprehensive reviews on current issues in neurosurgery. Each issue contains up to three reviews, reflecting all important aspects of one topic (a disease or a surgical approach). Comments by a panel of experts within the same issue complete the topic. By providing comprehensive coverage of one topic per issue, Neurosurgical Review combines the topicality of professional journals with the indepth treatment of a monograph. Original papers of high quality are also welcome.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


