Ana Margarida Martins, Joana Rigueira, Beatriz Valente Silva, Beatriz Nogueira Garcia, Pedro Alves da Silva, Ana Abrantes, Rui Plácido, Doroteia Silva, Fausto J Pinto, Ana G Almeida
{"title":"Calcium Hides the Clue: Unraveling the Diagnostic Value of Coronary Calcium Scoring in Cardiac Arrest Survivors.","authors":"Ana Margarida Martins, Joana Rigueira, Beatriz Valente Silva, Beatriz Nogueira Garcia, Pedro Alves da Silva, Ana Abrantes, Rui Plácido, Doroteia Silva, Fausto J Pinto, Ana G Almeida","doi":"10.3390/jpm15090422","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction</b>: Coronary artery disease remains one of the most prevalent causes of hospital cardiac arrest (OHCA). Although the benefit of early coronary angiography is well stablished in patients with ST-segment elevation, the benefit and the timing of performing it in other patients remain a matter of debate. This is due to the difficulty of identifying those in which an infarction with non-ST-segment elevation is the cause of the OHCA. Coronary artery calcium (CAC) emerges as a reliable predictor of coronary disease and adverse cardiovascular events, detectable even in non-gated chest computed tomography (CT) scans commonly used in OHCA etiological studies, showcasing potential for streamlined risk assessment and management. <b>Aim</b>: The aim of this study was to evaluate if CAC in non-gated CT scans performed in OHCA survivors could act as a good predictor of coronary artery disease on coronary angiography. <b>Methods</b>: This is a single-center, retrospective study of OHCA survivors without ST-segment elevation at presentation. We selected patients for whom a non-gated chest CT was performed and underwent coronary angiography due to the clinical, electrocardiogram (ECG), or echocardiographic suspicion of acute coronary syndrome. An investigator, blinded to the coronary angiography report, evaluated CAC both quantitively (with Agatston score) and qualitatively (visual assessment: absent, mild, moderate, or severe). <b>Results</b>: A total of 44 consecutive patients were included: 70% male, mean age of 60 ± 13 years old. The mean Agatston score was 396 ± 573 AU (Agatston units). Regarding the qualitative assessment, CAC was classified as mild, moderate, and severe in 11%, 25%, and 20% of patients, respectively. The coronary angiography revealed significant coronary lesions in 15 patients (34%), of which 87% were revascularized (80% underwent PCI and 7% CABG). The quantitative CAC assessment accurately predicted the presence of significant lesions on coronary angiography (AUC = 0.90, 95% CI 0.81-0.99, <i>p</i> < 0.001). The presence of moderate or severe CAC by visual assessment also predicted significant lesions on coronary angiography (OR 2.66, 95% CI 1.87-109.71, <i>p</i> = 0.01). There was also a good and significant correlation between the vessel with severe calcification in the CT scan and the culprit vessel evaluated by coronary angiography. CAC was reported in only 16% of the reviewed CTs, most of them with severe calcification. <b>Conclusion</b>: The assessment of CAC in non-gated chest CT scans proved to be feasible and displayed a robust correlation with the presence, severity, and location of coronary artery disease. Its routine use upfront was shown to be an important complement to CT scan reports, ensuring more precise and personalized OHCA management.</p>","PeriodicalId":16722,"journal":{"name":"Journal of Personalized Medicine","volume":"15 9","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2025-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12471230/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Personalized Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jpm15090422","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
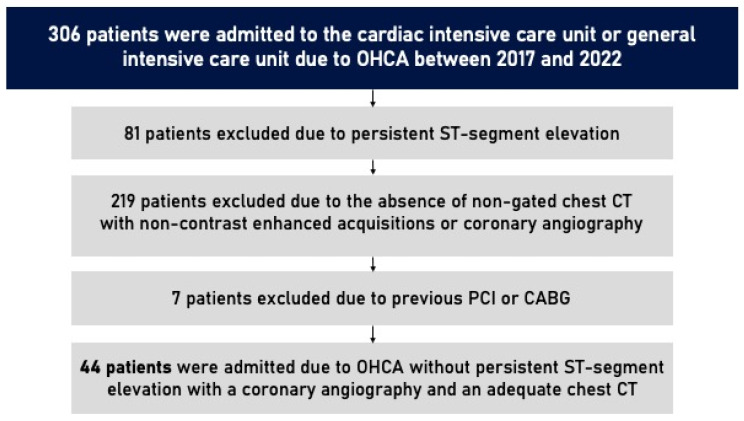
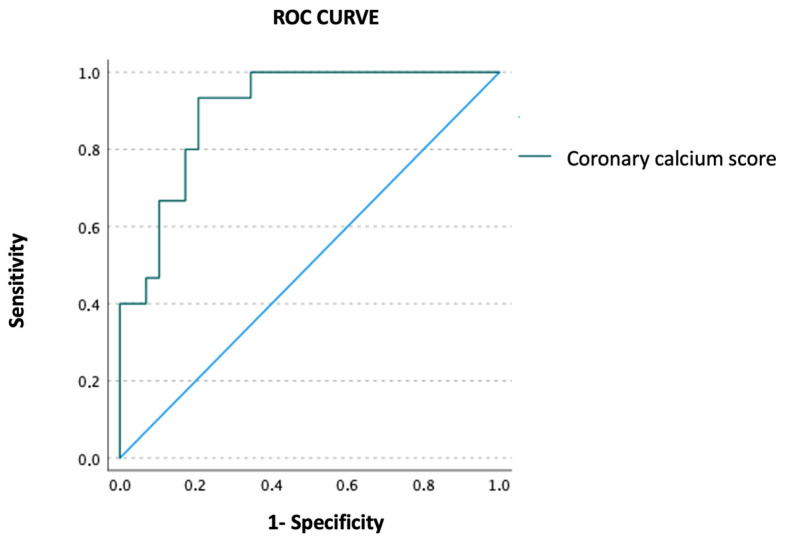
Introduction: Coronary artery disease remains one of the most prevalent causes of hospital cardiac arrest (OHCA). Although the benefit of early coronary angiography is well stablished in patients with ST-segment elevation, the benefit and the timing of performing it in other patients remain a matter of debate. This is due to the difficulty of identifying those in which an infarction with non-ST-segment elevation is the cause of the OHCA. Coronary artery calcium (CAC) emerges as a reliable predictor of coronary disease and adverse cardiovascular events, detectable even in non-gated chest computed tomography (CT) scans commonly used in OHCA etiological studies, showcasing potential for streamlined risk assessment and management. Aim: The aim of this study was to evaluate if CAC in non-gated CT scans performed in OHCA survivors could act as a good predictor of coronary artery disease on coronary angiography. Methods: This is a single-center, retrospective study of OHCA survivors without ST-segment elevation at presentation. We selected patients for whom a non-gated chest CT was performed and underwent coronary angiography due to the clinical, electrocardiogram (ECG), or echocardiographic suspicion of acute coronary syndrome. An investigator, blinded to the coronary angiography report, evaluated CAC both quantitively (with Agatston score) and qualitatively (visual assessment: absent, mild, moderate, or severe). Results: A total of 44 consecutive patients were included: 70% male, mean age of 60 ± 13 years old. The mean Agatston score was 396 ± 573 AU (Agatston units). Regarding the qualitative assessment, CAC was classified as mild, moderate, and severe in 11%, 25%, and 20% of patients, respectively. The coronary angiography revealed significant coronary lesions in 15 patients (34%), of which 87% were revascularized (80% underwent PCI and 7% CABG). The quantitative CAC assessment accurately predicted the presence of significant lesions on coronary angiography (AUC = 0.90, 95% CI 0.81-0.99, p < 0.001). The presence of moderate or severe CAC by visual assessment also predicted significant lesions on coronary angiography (OR 2.66, 95% CI 1.87-109.71, p = 0.01). There was also a good and significant correlation between the vessel with severe calcification in the CT scan and the culprit vessel evaluated by coronary angiography. CAC was reported in only 16% of the reviewed CTs, most of them with severe calcification. Conclusion: The assessment of CAC in non-gated chest CT scans proved to be feasible and displayed a robust correlation with the presence, severity, and location of coronary artery disease. Its routine use upfront was shown to be an important complement to CT scan reports, ensuring more precise and personalized OHCA management.
冠状动脉疾病仍然是医院心脏骤停(OHCA)最普遍的原因之一。尽管早期冠状动脉造影对st段抬高患者的益处已得到证实,但对其他患者的益处和时机仍存在争议。这是由于难以确定那些非st段抬高的梗死是OHCA的原因。冠状动脉钙(CAC)是冠状动脉疾病和不良心血管事件的可靠预测指标,即使在OHCA病因学研究中常用的非门控胸部计算机断层扫描(CT)中也能检测到,显示了简化风险评估和管理的潜力。目的:本研究的目的是评估在OHCA幸存者中进行的非门控CT扫描中的CAC是否可以作为冠状动脉造影中冠状动脉疾病的良好预测指标。方法:这是一项单中心,回顾性研究OHCA幸存者没有st段抬高的表现。我们选择了由于临床、心电图(ECG)或超声心动图怀疑急性冠状动脉综合征而行非门控胸部CT并行冠状动脉造影的患者。研究者对冠状动脉造影报告不知情,定量(Agatston评分)和定性(视觉评估:无、轻度、中度或重度)评估CAC。结果:共纳入连续44例患者:男性70%,平均年龄60±13岁。平均Agatston评分为396±573 AU (Agatston单位)。在定性评价方面,分别有11%、25%和20%的患者将CAC分为轻度、中度和重度。冠状动脉造影显示15例(34%)患者有明显的冠状动脉病变,其中87%进行了血运重建(80%行PCI, 7%行CABG)。定量CAC评估能准确预测冠状动脉造影中是否存在显著病变(AUC = 0.90, 95% CI 0.81-0.99, p < 0.001)。视觉评估中、重度CAC的存在也预示着冠状动脉造影的显著病变(or 2.66, 95% CI 1.87-109.71, p = 0.01)。CT扫描显示严重钙化的血管与冠状动脉造影评估的罪魁祸首血管也有很好的显著相关性。仅16%的ct报告了CAC,其中大多数伴有严重的钙化。结论:在非门控胸部CT扫描中评估CAC被证明是可行的,并且与冠状动脉疾病的存在、严重程度和位置有很强的相关性。它的常规使用被证明是CT扫描报告的重要补充,确保更精确和个性化的OHCA管理。
期刊介绍:
Journal of Personalized Medicine (JPM; ISSN 2075-4426) is an international, open access journal aimed at bringing all aspects of personalized medicine to one platform. JPM publishes cutting edge, innovative preclinical and translational scientific research and technologies related to personalized medicine (e.g., pharmacogenomics/proteomics, systems biology). JPM recognizes that personalized medicine—the assessment of genetic, environmental and host factors that cause variability of individuals—is a challenging, transdisciplinary topic that requires discussions from a range of experts. For a comprehensive perspective of personalized medicine, JPM aims to integrate expertise from the molecular and translational sciences, therapeutics and diagnostics, as well as discussions of regulatory, social, ethical and policy aspects. We provide a forum to bring together academic and clinical researchers, biotechnology, diagnostic and pharmaceutical companies, health professionals, regulatory and ethical experts, and government and regulatory authorities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


