{"title":"Development and validation of a nomogram to predict the risk of type II endoleak after endovascular aneurysm repair.","authors":"Bowen Liu, Xiaobin Tang, Nan He, Zhong Chen","doi":"10.3389/fcvm.2025.1639697","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Type II endoleak (T2EL) is the most common complication following endovascular aneurysm repair (EVAR) of abdominal aortic aneurysms (AAA). T2EL may lead to aneurysm sac expansion and rupture. Identifying high-risk patients is crucial for prophylaxis and early intervention.</p><p><strong>Methods: </strong>This single-center retrospective study included 332 patients who underwent EVAR for infrarenal AAA. Demographic, clinical, anatomical, and medication-related data were collected. A nomogram was developed based on significant predictors. Its performance was assessed by receiver operating characteristic (ROC) curves, calibration plots, and decision curve analysis (DCA).</p><p><strong>Results: </strong>T2EL occurred in 70 (21.08%) of 332 patients. Multivariate logistic regression revealed six independent predictors: age, smoking status, intraluminal thrombus (ILT), number of patent lumbar arteries (LA), inferior mesenteric artery (IMA) diameter, and IMA patency. The nomogram demonstrated excellent calibration and strong predictive ability, with an area under the curve (AUC) of 0.806 (training set) and 0.758 (validation set). DCA showed clinical benefit across threshold probabilities of 1%-66% and 79%-92% in the training set, and 1%-84% in the validation set.</p><p><strong>Conclusion: </strong>The proposed nomogram effectively integrates clinical and anatomical factors to assess the risk of T2EL after EVAR. It may help identify patients requiring intensified surveillance or early interventions to mitigate complications. Further multicenter, prospective studies are needed to validate the nomogram's applicability.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"12 ","pages":"1639697"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12457305/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2025.1639697","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Type II endoleak (T2EL) is the most common complication following endovascular aneurysm repair (EVAR) of abdominal aortic aneurysms (AAA). T2EL may lead to aneurysm sac expansion and rupture. Identifying high-risk patients is crucial for prophylaxis and early intervention.
Methods: This single-center retrospective study included 332 patients who underwent EVAR for infrarenal AAA. Demographic, clinical, anatomical, and medication-related data were collected. A nomogram was developed based on significant predictors. Its performance was assessed by receiver operating characteristic (ROC) curves, calibration plots, and decision curve analysis (DCA).
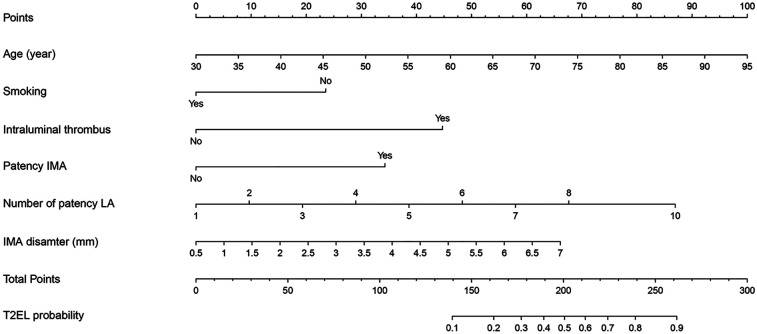
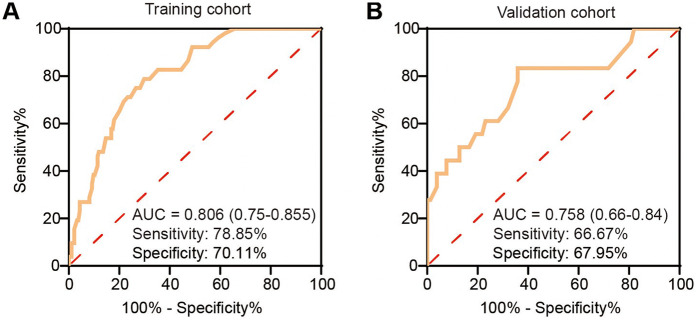
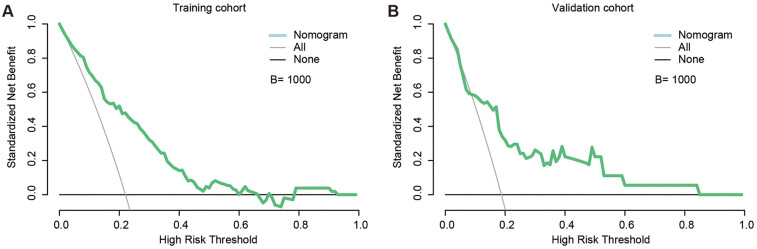
Results: T2EL occurred in 70 (21.08%) of 332 patients. Multivariate logistic regression revealed six independent predictors: age, smoking status, intraluminal thrombus (ILT), number of patent lumbar arteries (LA), inferior mesenteric artery (IMA) diameter, and IMA patency. The nomogram demonstrated excellent calibration and strong predictive ability, with an area under the curve (AUC) of 0.806 (training set) and 0.758 (validation set). DCA showed clinical benefit across threshold probabilities of 1%-66% and 79%-92% in the training set, and 1%-84% in the validation set.
Conclusion: The proposed nomogram effectively integrates clinical and anatomical factors to assess the risk of T2EL after EVAR. It may help identify patients requiring intensified surveillance or early interventions to mitigate complications. Further multicenter, prospective studies are needed to validate the nomogram's applicability.
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


