{"title":"Role of peri-deployment right ventricular paced-ECG in left bundle area pacing.","authors":"Wen-De Tang, Chiung-Ray Lu, Mei-Yao Wu, Ching-Fen Chang, Wei-Hsin Chung, Yin-Huei Chen, Hung-Pin Wu, Hei-Tung Yip, Kuan-Cheng Chang, Yen-Nien Lin","doi":"10.3389/fcvm.2025.1555683","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Left bundle area pacing (LBBAP) has emerged as a promising physiological pacing modality. The current technique for LBBAP lead implantation predominantly relies on the anatomy of the His bundle and right ventricular septum. While practical, this anatomical approach can lead to variations in lead polarity and QRS durations due to the relatively extensive target zone.</p><p><strong>Objectives: </strong>This study aims to investigate whether peri-deployment paced ECGs can effectively guide LBBAP and enhance left ventricular activation.</p><p><strong>Methods: </strong>We conducted a retrospective analysis of 41 patients (54 attempts) who underwent LBBAP between 1 September 2020 and 30 June 2021. We collected and analyzed demographic data, baseline ECGs, intraprocedural ECGs, and ventricular local electrograms. QRS patterns were categorized into five common types, R, Rs, rs, rS, and S, and were labeled from 1 to 5 for polarity analysis. In addition, we explored markers associated with achieving shorter QRS durations (<120 ms).</p><p><strong>Results: </strong>LBBAP was successfully achieved in 81.5% of the attempts. During the procedure, the paced QRS duration (QRSd) significantly decreased from 144.5 ± 22.6 ms-128.8 ± 22.9 ms (<i>p</i> < 0.001). Comparing lead polarity scores before and after deployment revealed a significant increase in leads I and aVL (lead I, 1.3 ± 0.9 vs. 1.6 ± 1.0, <i>p</i> = 0.002; lead aVL, 1.6 ± 1.0 vs. 2.1 ± 1.3, <i>p</i> = 0.002), while leads III and aVF showed a decrease (lead III, 3.9 ± 1.2 vs. 3.4 ± 1.5, <i>p</i> = 0.001; lead aVF, 3.1 ± 1.2 vs. 2.9 ± 1.3, <i>p</i> = 0.026). The polarity of leads II and aVR remained unchanged. In the subgroup with post-deployment QRSd shorter than 120 ms, although the Qr pattern in lead V1 was only numerically higher (95.2% vs. 81.8%, <i>p</i> = 0.310), the lead polarity scores were significantly higher in leads I and aVL and lower in leads III and aVF (<i>p</i> < 0.001). This group also had a significantly shorter left ventricular activation time (LVAT) (68.7 ± 13.0 ms vs. 98.4 ± 14.0 ms, <i>p</i> < 0.001). Univariate analysis revealed that a shorter pre-deployment paced QRSd and LVAT were associated with a narrower post-deployment QRSd. In addition, non-electrical factors such as female gender and left ventricular dilation were associated with higher post-deployment QRSd.</p><p><strong>Conclusions: </strong>Peri-deployment ECG assessment is a practical adjunct to anatomy-based LBBAP, providing real-time markers for optimal lead positioning. Specifically, an unaltered lead II axis and expected changes in the lead I/aVL and lead III/aVF axes can help guide the selection of the left bundle branch. Lower pre-deployment paced QRSd and LVAT, as well as a more rightward inferior axis after deployment, are associated with a shorter post-deployment QRSd.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"12 ","pages":"1555683"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12457291/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2025.1555683","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Left bundle area pacing (LBBAP) has emerged as a promising physiological pacing modality. The current technique for LBBAP lead implantation predominantly relies on the anatomy of the His bundle and right ventricular septum. While practical, this anatomical approach can lead to variations in lead polarity and QRS durations due to the relatively extensive target zone.
Objectives: This study aims to investigate whether peri-deployment paced ECGs can effectively guide LBBAP and enhance left ventricular activation.
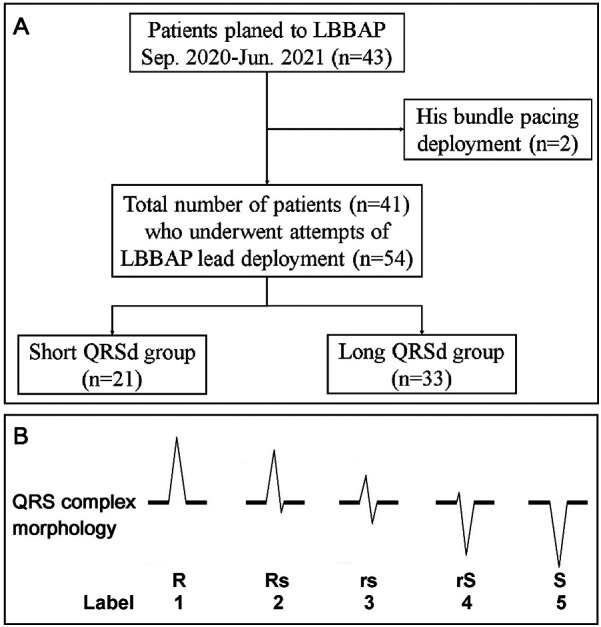
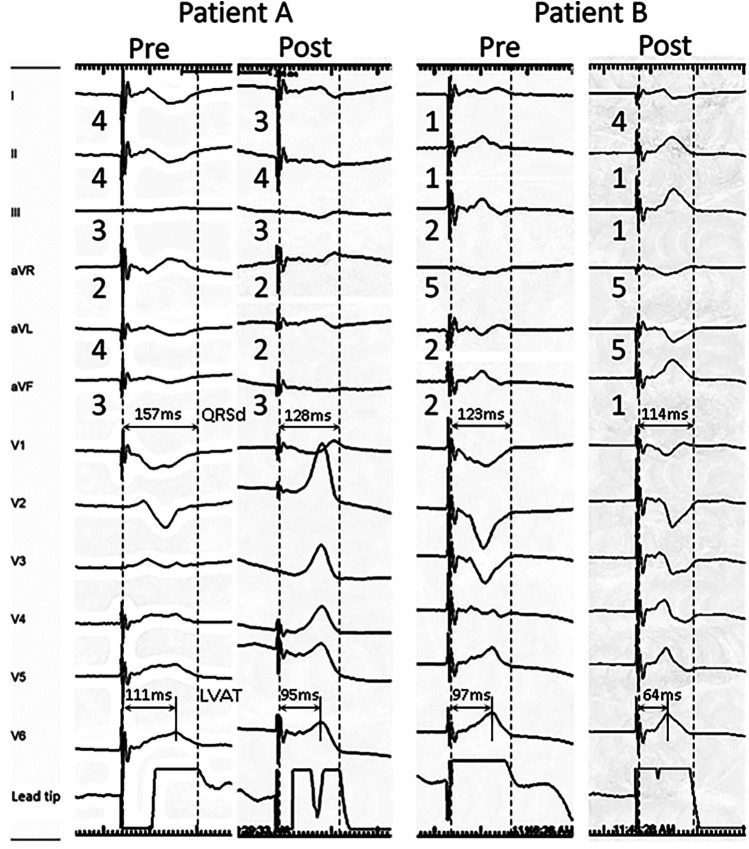
Methods: We conducted a retrospective analysis of 41 patients (54 attempts) who underwent LBBAP between 1 September 2020 and 30 June 2021. We collected and analyzed demographic data, baseline ECGs, intraprocedural ECGs, and ventricular local electrograms. QRS patterns were categorized into five common types, R, Rs, rs, rS, and S, and were labeled from 1 to 5 for polarity analysis. In addition, we explored markers associated with achieving shorter QRS durations (<120 ms).
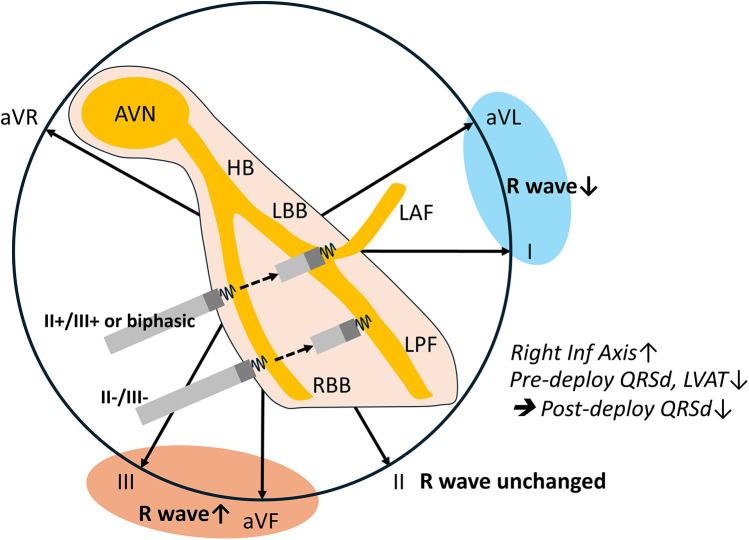
Results: LBBAP was successfully achieved in 81.5% of the attempts. During the procedure, the paced QRS duration (QRSd) significantly decreased from 144.5 ± 22.6 ms-128.8 ± 22.9 ms (p < 0.001). Comparing lead polarity scores before and after deployment revealed a significant increase in leads I and aVL (lead I, 1.3 ± 0.9 vs. 1.6 ± 1.0, p = 0.002; lead aVL, 1.6 ± 1.0 vs. 2.1 ± 1.3, p = 0.002), while leads III and aVF showed a decrease (lead III, 3.9 ± 1.2 vs. 3.4 ± 1.5, p = 0.001; lead aVF, 3.1 ± 1.2 vs. 2.9 ± 1.3, p = 0.026). The polarity of leads II and aVR remained unchanged. In the subgroup with post-deployment QRSd shorter than 120 ms, although the Qr pattern in lead V1 was only numerically higher (95.2% vs. 81.8%, p = 0.310), the lead polarity scores were significantly higher in leads I and aVL and lower in leads III and aVF (p < 0.001). This group also had a significantly shorter left ventricular activation time (LVAT) (68.7 ± 13.0 ms vs. 98.4 ± 14.0 ms, p < 0.001). Univariate analysis revealed that a shorter pre-deployment paced QRSd and LVAT were associated with a narrower post-deployment QRSd. In addition, non-electrical factors such as female gender and left ventricular dilation were associated with higher post-deployment QRSd.
Conclusions: Peri-deployment ECG assessment is a practical adjunct to anatomy-based LBBAP, providing real-time markers for optimal lead positioning. Specifically, an unaltered lead II axis and expected changes in the lead I/aVL and lead III/aVF axes can help guide the selection of the left bundle branch. Lower pre-deployment paced QRSd and LVAT, as well as a more rightward inferior axis after deployment, are associated with a shorter post-deployment QRSd.
背景:左束区起搏(LBBAP)已成为一种很有前途的生理起搏方式。目前的LBBAP引线植入技术主要依赖于他束和右室间隔的解剖。虽然实用,但由于相对广泛的靶区,这种解剖方法可能导致导联极性和QRS持续时间的变化。目的:本研究旨在探讨围部署期起搏心电图是否能有效引导LBBAP,增强左心室激活。方法:我们对2020年9月1日至2021年6月30日期间接受LBBAP的41例患者(54次尝试)进行了回顾性分析。我们收集并分析了人口统计学数据、基线心电图、术中心电图和心室局部心电图。QRS模式分为R、Rs、Rs、Rs和S五种常见类型,并从1到5进行极性分析。此外,我们探索了与获得更短QRS持续时间相关的标记(结果:81.5%的尝试成功实现了LBBAP。QRSd从144.5±22.6 ms降至128.8±22.9 ms (p = 0.002; aVL导联为1.6±1.0 vs. 2.1±1.3,p = 0.002), aVF导联为3.1±1.2 vs. 3.4±1.5,p = 0.001; aVF导联为3.1±1.2 vs. 2.9±1.3,p = 0.026)。导联II和aVR的极性保持不变。在部署后QRSd短于120 ms的亚组中,尽管V1导联的Qr模式仅在数值上较高(95.2% vs. 81.8%, p = 0.310),但导联I和aVL的导联极性得分明显较高,导联III和aVF的导联极性得分明显较低(p结论:部署前后心电图评估是基于解剖的LBBAP的实用辅助,为最佳导联定位提供了实时标记。具体来说,未改变的导联II轴和导联I/aVL和导联III/aVF轴的预期变化有助于指导左束分支的选择。较低的部署前QRSd和LVAT,以及部署后更向右的下轴,与较短的部署后QRSd相关。
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


