{"title":"Mercury exposure leading to functional vitamin B12 deficiency and subacute combined degeneration: a case report and literature review.","authors":"Isidora Semnic, Valentino Rački, Olivia Perković, Vladimira Vuletić","doi":"10.3389/ftox.2025.1580275","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The association between neurological symptomatology and heavy metal exposure has been reported in the literature. A few cases of extrapyramidal symptomatology and subacute combined degeneration have been described as manifestations of mercury intoxication. We highlight a case of a patient presenting with Parkinsonian features (tremor, rigidity, and bradykinesia), pyramidal deficits, dysarthria, paresthesia, mild cognitive decline, and emotional lability, with proven elevated mercury levels in blood and hair and elevated arsenic in urine.</p><p><strong>Case: </strong>A 60-year-old man, with history of mercury exposure while working at the Centre for Waste Management and Environmental Protection presented to a neurologist after 10 months of persistent tremors, muscle spasms, paresthesia, and irritability, followed by the onset of bradykinesia, slurred speech, rigidity, insomnia, and subtle cognitive decline. Laboratory investigations revealed functional vitamin B12 and vitamin D deficiencies, while toxicological quantitative analysis showed elevated blood mercury levels (15.2 μg/L) and hair root levels (3 μg/g). MRI of the brain was normal, whereas MRI of the posterior cervical spine detected signs of myelopathy. Florodeoxyglucose (FDG) Positron Emission Tomography (PET) of the brain revealed bilateral temporal and parietal glucose hypometabolism, most pronounced in the left inferior parietal and left superior temporal regions. Single-Photon Emission Computed Tomography (SPECT) imaging of dopaminergic neurons in the striatum was negative, and the patient was unresponsive to levodopa. Multivitamin therapy (vitamins B, E, and D) with selenium, in combination with symptomatic therapy (benzodiazepines, muscle relaxants, and antidepressants) provided minimal relief, leading to the introduction of N-acetyl cysteine, which resulted in moderate improvement of symptoms. Physical and speech therapy were of great importance in this case.</p><p><strong>Discussion: </strong>This case is unique because it represents the development of therapy-resistant extrapyramidal symptoms over 3 years of mercury exposure, likely leading to subacute combined degeneration due to functional vitamin B12 deficiency. Epidemiological data describe methylmercury poisoning, known as Minamata disease, which presents with -somatosensory deficits, ataxia, parkinsonism, dysarthria, and visual and hearing impairments.</p><p><strong>Conclusion: </strong>Toxicological screening for heavy metals in blood and urine should be considered in patients presenting with unexplained, levodopa-resistant extrapyramidal symptoms, behavioral and sleep disturbances, cognitive decline, and other non-specific neurological signs.</p>","PeriodicalId":73111,"journal":{"name":"Frontiers in toxicology","volume":"7 ","pages":"1580275"},"PeriodicalIF":4.6000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12454407/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in toxicology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/ftox.2025.1580275","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"TOXICOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The association between neurological symptomatology and heavy metal exposure has been reported in the literature. A few cases of extrapyramidal symptomatology and subacute combined degeneration have been described as manifestations of mercury intoxication. We highlight a case of a patient presenting with Parkinsonian features (tremor, rigidity, and bradykinesia), pyramidal deficits, dysarthria, paresthesia, mild cognitive decline, and emotional lability, with proven elevated mercury levels in blood and hair and elevated arsenic in urine.
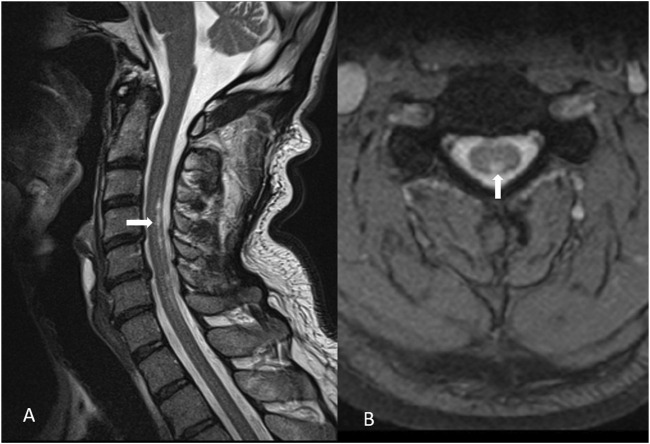
Case: A 60-year-old man, with history of mercury exposure while working at the Centre for Waste Management and Environmental Protection presented to a neurologist after 10 months of persistent tremors, muscle spasms, paresthesia, and irritability, followed by the onset of bradykinesia, slurred speech, rigidity, insomnia, and subtle cognitive decline. Laboratory investigations revealed functional vitamin B12 and vitamin D deficiencies, while toxicological quantitative analysis showed elevated blood mercury levels (15.2 μg/L) and hair root levels (3 μg/g). MRI of the brain was normal, whereas MRI of the posterior cervical spine detected signs of myelopathy. Florodeoxyglucose (FDG) Positron Emission Tomography (PET) of the brain revealed bilateral temporal and parietal glucose hypometabolism, most pronounced in the left inferior parietal and left superior temporal regions. Single-Photon Emission Computed Tomography (SPECT) imaging of dopaminergic neurons in the striatum was negative, and the patient was unresponsive to levodopa. Multivitamin therapy (vitamins B, E, and D) with selenium, in combination with symptomatic therapy (benzodiazepines, muscle relaxants, and antidepressants) provided minimal relief, leading to the introduction of N-acetyl cysteine, which resulted in moderate improvement of symptoms. Physical and speech therapy were of great importance in this case.
Discussion: This case is unique because it represents the development of therapy-resistant extrapyramidal symptoms over 3 years of mercury exposure, likely leading to subacute combined degeneration due to functional vitamin B12 deficiency. Epidemiological data describe methylmercury poisoning, known as Minamata disease, which presents with -somatosensory deficits, ataxia, parkinsonism, dysarthria, and visual and hearing impairments.
Conclusion: Toxicological screening for heavy metals in blood and urine should be considered in patients presenting with unexplained, levodopa-resistant extrapyramidal symptoms, behavioral and sleep disturbances, cognitive decline, and other non-specific neurological signs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


