Marta Marcos-Mangas, Teresa López-Sobrino, Albert Ariza-Solé, Ferran Rueda-Sobella, Esther Sanz-Girgas, Jaime Aboal, Pablo Pastor, Irene Buera, Alessandro Sionis, Rut Andrea, Judit Rodríguez-López, Carlos Tomas, Jordi Bañeras, Isaac Llaó, José Carlos Sánchez-Salado, Cosme Garcia-Garcia
{"title":"Socioeconomic status and equity among patients with cardiogenic shock.","authors":"Marta Marcos-Mangas, Teresa López-Sobrino, Albert Ariza-Solé, Ferran Rueda-Sobella, Esther Sanz-Girgas, Jaime Aboal, Pablo Pastor, Irene Buera, Alessandro Sionis, Rut Andrea, Judit Rodríguez-López, Carlos Tomas, Jordi Bañeras, Isaac Llaó, José Carlos Sánchez-Salado, Cosme Garcia-Garcia","doi":"10.3389/fcvm.2025.1597225","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We aimed to analyze the impact of socioeconomic status (SES) on management and in-hospital outcomes of patients with cardiogenic shock (CS).</p><p><strong>Methods: </strong>This was a prospective observational registry conducted (December 2018-November 2019) in Intensive Cardiac Care Units (ICCU) across 8 tertiary care centers. Consecutive patients aged ≥18 years with a primary diagnosis of cardiogenic shock were included. SES was defined using a numerical index that incorporates mean income levels, premature mortality, and avoidable hospitalizations observed within a specific health area. SES values were categorized into tertiles. In-hospital procedures, complications, length of stay, and in-hospital mortality were collected.</p><p><strong>Results: </strong>A total of 382 patients were included (mean age: 65.3 years). There were no differences in age, sex, or major comorbidities across SES groups. CS was more frequently due to acute coronary syndrome (ACS) in patients with low SES (66.9% vs. 58%, <i>p</i> = 0.022). No significant differences were observed regarding SCAI stage or other severity markers of CS across SES groups. Patients with low SES were more likely to receive pulmonary artery catheterization (<i>p</i> = 0.029) and mechanical circulatory support (<i>p</i> = 0.038). After adjusting for potential confounders, clinical management was similar regardless SES. Lower SES patients exhibited a higher incidence of bleeding (<i>p</i> = 0.018). There were no differences in length of stay or in-hospital mortality among SES groups.</p><p><strong>Conclusions: </strong>Beyond a higher rate of ACS-related CS, patients with low SES exhibited a clinical profile and shock severity comparable to other SES groups. Therapeutic management aligned with guideline recommendations even in patients with low SES.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"12 ","pages":"1597225"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12454308/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2025.1597225","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: We aimed to analyze the impact of socioeconomic status (SES) on management and in-hospital outcomes of patients with cardiogenic shock (CS).
Methods: This was a prospective observational registry conducted (December 2018-November 2019) in Intensive Cardiac Care Units (ICCU) across 8 tertiary care centers. Consecutive patients aged ≥18 years with a primary diagnosis of cardiogenic shock were included. SES was defined using a numerical index that incorporates mean income levels, premature mortality, and avoidable hospitalizations observed within a specific health area. SES values were categorized into tertiles. In-hospital procedures, complications, length of stay, and in-hospital mortality were collected.
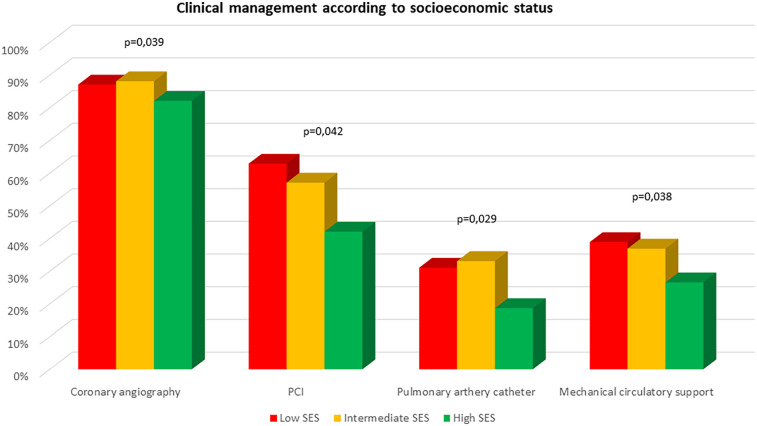
Results: A total of 382 patients were included (mean age: 65.3 years). There were no differences in age, sex, or major comorbidities across SES groups. CS was more frequently due to acute coronary syndrome (ACS) in patients with low SES (66.9% vs. 58%, p = 0.022). No significant differences were observed regarding SCAI stage or other severity markers of CS across SES groups. Patients with low SES were more likely to receive pulmonary artery catheterization (p = 0.029) and mechanical circulatory support (p = 0.038). After adjusting for potential confounders, clinical management was similar regardless SES. Lower SES patients exhibited a higher incidence of bleeding (p = 0.018). There were no differences in length of stay or in-hospital mortality among SES groups.
Conclusions: Beyond a higher rate of ACS-related CS, patients with low SES exhibited a clinical profile and shock severity comparable to other SES groups. Therapeutic management aligned with guideline recommendations even in patients with low SES.
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


