Efficacy and safety of short-acting β-blockers in patients with sepsis-associated cardiac dysfunction: a systematic review and meta-analysis of randomized controlled trials.
Min'an Zheng, Jin Wang, Pingchang Xie, Shijun Guo, Benjian Chen, Zhuogen He, Guoyan Yao
{"title":"Efficacy and safety of short-acting β-blockers in patients with sepsis-associated cardiac dysfunction: a systematic review and meta-analysis of randomized controlled trials.","authors":"Min'an Zheng, Jin Wang, Pingchang Xie, Shijun Guo, Benjian Chen, Zhuogen He, Guoyan Yao","doi":"10.3389/fcvm.2025.1665466","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The role of ultra-rapid β-blockers in sepsis-associated cardiac dysfunction remains controversial, with conflicting evidence regarding mortality benefits and safety concerns in hemodynamically unstable patients.</p><p><strong>Methods: </strong>This study retrieved relevant reports on randomized controlled trials of ultra-rapid β-blockers conducted for adult patients with sepsis-associated cardiac dysfunction, up to and including the date of May 30, 2025, from the databases of PubMed, Web of Science, Cochrane Library and Embase. Primary outcomes were 28-day mortality and adverse events; secondary outcomes included heart rate control and mean arterial pressure (MAP) at 48 h. Random-effects models calculated risk ratios (RR) or standardized mean differences (SMD) with 95% confidence intervals (CI). Heterogeneity was assessed using I² statistics.</p><p><strong>Results: </strong>Eight studies reported 28-day mortality, showing no significant reduction with ultra-rapid β-blockers (RR, 0.84, 95% CI: 0.67-1.06; <i>P</i> = 0.15; I² = 54%). Safety data from four studies indicated no increased adverse events (RR, 1.04, 95% CI: 0.82-1.33; <i>P</i> = 0.72; I² = 0%). Paradoxically, ultra-rapid β-blockers were associated with worse heart rate control (RR, 1.51, 95% CI: 1.00-2.29; <i>P</i> = 0.05). MAP at 48 h showed no intergroup difference (SMD, -0.85, 95% CI: -2.24-0.54).</p><p><strong>Conclusion: </strong>ultra-rapid β-blockers demonstrate an acceptable safety profile without compromising hemodynamic stability but fail to reduce 28-day mortality in sepsis-associated cardiac dysfunction patients. The inferior heart rate control suggests potential physiological incompatibility in this population. Precision targeting based on adrenergic activity and cardiac phenotyping warrants investigation.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"12 ","pages":"1665466"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12454437/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2025.1665466","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The role of ultra-rapid β-blockers in sepsis-associated cardiac dysfunction remains controversial, with conflicting evidence regarding mortality benefits and safety concerns in hemodynamically unstable patients.
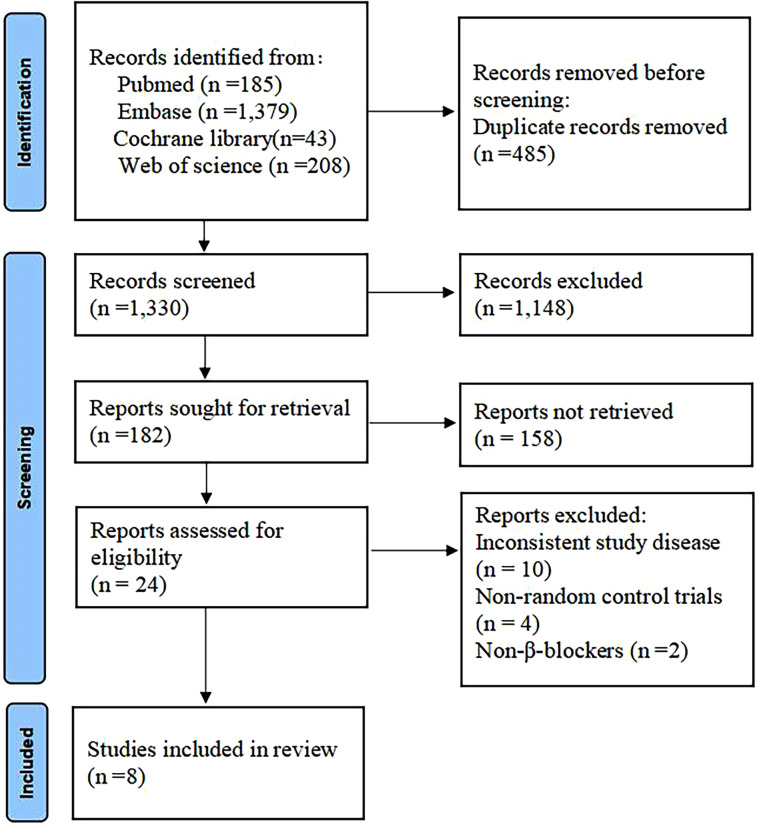
Methods: This study retrieved relevant reports on randomized controlled trials of ultra-rapid β-blockers conducted for adult patients with sepsis-associated cardiac dysfunction, up to and including the date of May 30, 2025, from the databases of PubMed, Web of Science, Cochrane Library and Embase. Primary outcomes were 28-day mortality and adverse events; secondary outcomes included heart rate control and mean arterial pressure (MAP) at 48 h. Random-effects models calculated risk ratios (RR) or standardized mean differences (SMD) with 95% confidence intervals (CI). Heterogeneity was assessed using I² statistics.
Results: Eight studies reported 28-day mortality, showing no significant reduction with ultra-rapid β-blockers (RR, 0.84, 95% CI: 0.67-1.06; P = 0.15; I² = 54%). Safety data from four studies indicated no increased adverse events (RR, 1.04, 95% CI: 0.82-1.33; P = 0.72; I² = 0%). Paradoxically, ultra-rapid β-blockers were associated with worse heart rate control (RR, 1.51, 95% CI: 1.00-2.29; P = 0.05). MAP at 48 h showed no intergroup difference (SMD, -0.85, 95% CI: -2.24-0.54).
Conclusion: ultra-rapid β-blockers demonstrate an acceptable safety profile without compromising hemodynamic stability but fail to reduce 28-day mortality in sepsis-associated cardiac dysfunction patients. The inferior heart rate control suggests potential physiological incompatibility in this population. Precision targeting based on adrenergic activity and cardiac phenotyping warrants investigation.
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


