Victoria García-Martín, MCanto de Hoyos-Alonso, Jesús Martín-Fernández, Isabel Del Cura-González
{"title":"Mortality and institutionalization of patients with dementia treated in primary care: influence of neuropsychiatric symptoms (NeDEM project).","authors":"Victoria García-Martín, MCanto de Hoyos-Alonso, Jesús Martín-Fernández, Isabel Del Cura-González","doi":"10.1186/s12877-025-06339-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neuropsychiatric symptoms (NPSs) are common in people with dementia (PWD), but their associations with the risk of institutionalization and mortality are controversial. The objective of this study was to estimate the incidence of institutionalization and death among PWD treated in primary care (PC) and to analyse the associations between NPSs and these events.</p><p><strong>Methods: </strong>This was a longitudinal analytical observational study of PWD in PC with a 4-year follow-up. Data on sociodemographic, clinical and functional characteristics and prescribed treatments for dementia were collected. NPSs were examined with the Neuropsychiatric Inventory (NPI) scale and according to the presence of clinically relevant neuropsychiatric subsyndromes. The incidence of institutionalization and cumulative mortality were calculated annually and at four years. Survival analysis with Kaplan‒Meier curves and Cox regression was performed to analyse the influence of NPSs on institutionalization and mortality.</p><p><strong>Results: </strong>A total of 124 patients with a mean age of 82.5 (8.0) years were included, and 69.4% were women. At four years, the institutionalization rate in a nursing home was 29.8% (95% CI 22.0; 38.7), with a median time to institutionalization of 13.2 months (IQR: 6.8-31.5). The mortality rate was 48.4% (95% CI 39.3; 57.5), with a median survival time of 21.7 months (IQR: 14.2-32.0). The NPI score was associated with institutionalization (HR 1.27, 95% CI 1.12, 1.45) and mortality (HR 1.47, 95% CI 1.40, 1.54). Among the subsyndromes, the presence of clinically relevant apathy was associated with institutionalization (HR 2.23, 95% CI 1.29, 3.88) and mortality (HR 1.56, 95% CI 1.34, 1.81).</p><p><strong>Conclusions: </strong>In PWD who were followed up in the community for four years, one-third of the patients were institutionalized, and half died. The intensity of the NPSs influences both institutionalization and mortality, with subsyndrome apathy (formed by the symptoms of apathy and appetite alterations) being the one that most influences both outcomes.</p>","PeriodicalId":9056,"journal":{"name":"BMC Geriatrics","volume":"25 1","pages":"701"},"PeriodicalIF":3.8000,"publicationDate":"2025-09-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12462034/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Geriatrics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12877-025-06339-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Neuropsychiatric symptoms (NPSs) are common in people with dementia (PWD), but their associations with the risk of institutionalization and mortality are controversial. The objective of this study was to estimate the incidence of institutionalization and death among PWD treated in primary care (PC) and to analyse the associations between NPSs and these events.
Methods: This was a longitudinal analytical observational study of PWD in PC with a 4-year follow-up. Data on sociodemographic, clinical and functional characteristics and prescribed treatments for dementia were collected. NPSs were examined with the Neuropsychiatric Inventory (NPI) scale and according to the presence of clinically relevant neuropsychiatric subsyndromes. The incidence of institutionalization and cumulative mortality were calculated annually and at four years. Survival analysis with Kaplan‒Meier curves and Cox regression was performed to analyse the influence of NPSs on institutionalization and mortality.
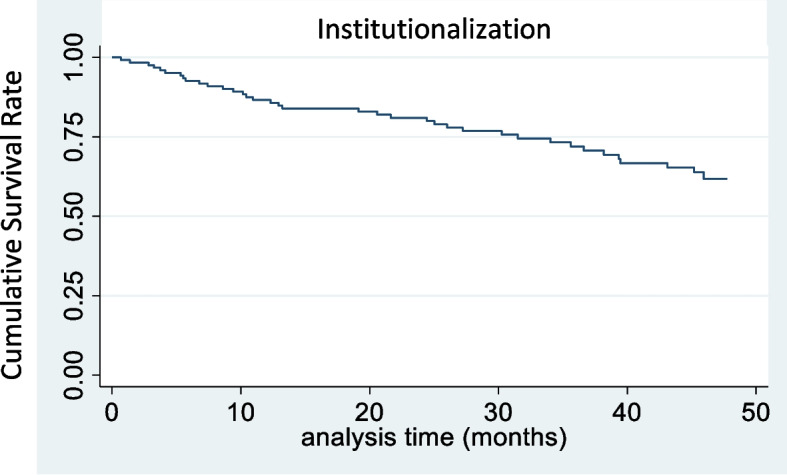
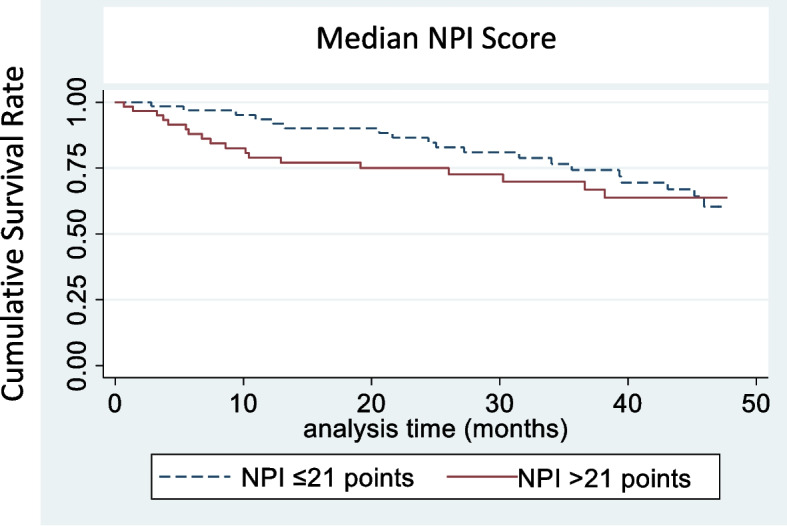
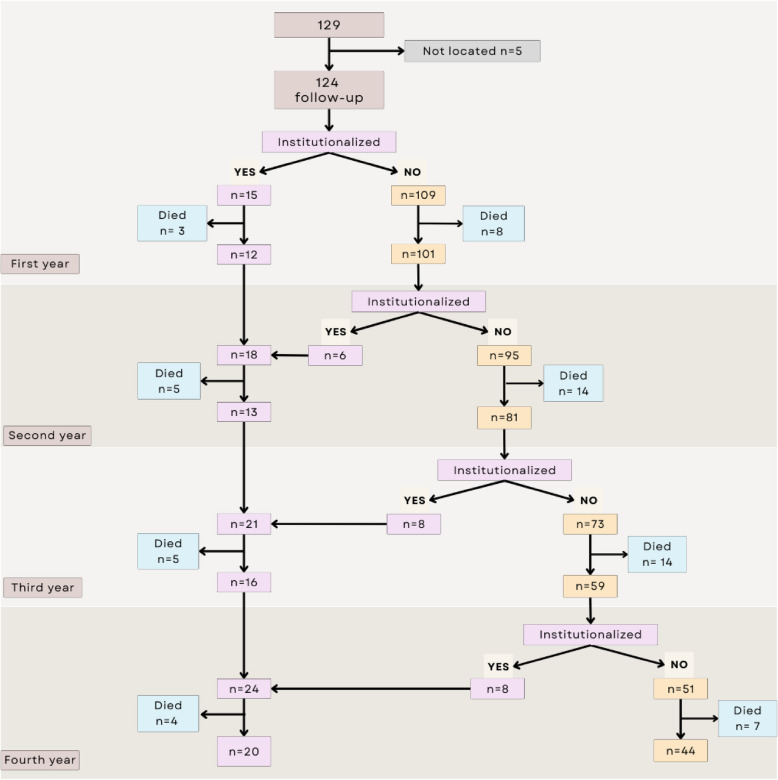
Results: A total of 124 patients with a mean age of 82.5 (8.0) years were included, and 69.4% were women. At four years, the institutionalization rate in a nursing home was 29.8% (95% CI 22.0; 38.7), with a median time to institutionalization of 13.2 months (IQR: 6.8-31.5). The mortality rate was 48.4% (95% CI 39.3; 57.5), with a median survival time of 21.7 months (IQR: 14.2-32.0). The NPI score was associated with institutionalization (HR 1.27, 95% CI 1.12, 1.45) and mortality (HR 1.47, 95% CI 1.40, 1.54). Among the subsyndromes, the presence of clinically relevant apathy was associated with institutionalization (HR 2.23, 95% CI 1.29, 3.88) and mortality (HR 1.56, 95% CI 1.34, 1.81).
Conclusions: In PWD who were followed up in the community for four years, one-third of the patients were institutionalized, and half died. The intensity of the NPSs influences both institutionalization and mortality, with subsyndrome apathy (formed by the symptoms of apathy and appetite alterations) being the one that most influences both outcomes.
背景:神经精神症状(nps)在痴呆症(PWD)患者中很常见,但其与住院风险和死亡率的关系存在争议。本研究的目的是估计在初级保健(PC)中接受治疗的PWD的机构化和死亡发生率,并分析nps与这些事件之间的关系。方法:这是一项对PC患者PWD进行的纵向分析观察研究,随访4年。收集痴呆的社会人口学、临床和功能特征以及处方治疗的数据。采用神经精神量表(NPI)并根据临床相关神经精神亚综合征的存在对nps进行检查。每年和每四年计算住院率和累计死亡率。采用Kaplan-Meier曲线和Cox回归进行生存分析,分析nps对住院和死亡率的影响。结果:共纳入124例患者,平均年龄82.5(8.0)岁,其中69.4%为女性。四年后,养老院的住院率为29.8% (95% CI 22.0; 38.7),中位住院时间为13.2个月(IQR: 6.8-31.5)。死亡率为48.4% (95% CI 39.3; 57.5),中位生存时间为21.7个月(IQR: 14.2-32.0)。NPI评分与住院(HR 1.27, 95% CI 1.12, 1.45)和死亡率(HR 1.47, 95% CI 1.40, 1.54)相关。在亚综合征中,临床相关冷漠的存在与住院(相对危险度2.23,95% CI 1.29, 3.88)和死亡率(相对危险度1.56,95% CI 1.34, 1.81)相关。结论:在社区随访4年的PWD患者中,三分之一的患者住院,一半死亡。nps的强度影响着住院和死亡率,而亚综合征冷漠(由冷漠和食欲改变的症状形成)是对这两种结果影响最大的一个。
期刊介绍:
BMC Geriatrics is an open access journal publishing original peer-reviewed research articles in all aspects of the health and healthcare of older people, including the effects of healthcare systems and policies. The journal also welcomes research focused on the aging process, including cellular, genetic, and physiological processes and cognitive modifications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


