Association of disease-modifying antirheumatic drug selection with hospitalised infection among youth with childhood-onset systemic lupus erythematosus.
Jordan E Roberts, Anna V Faino, Marshall Brown, Gabrielle Alonzi, Mersine A Bryan, Cordelia Burn, Joyce C Chang, Jonathan D Cogen, Nidhi Naik, Kareena Patel, Emily Zhang, Esi M Morgan, MaryBeth Son
{"title":"Association of disease-modifying antirheumatic drug selection with hospitalised infection among youth with childhood-onset systemic lupus erythematosus.","authors":"Jordan E Roberts, Anna V Faino, Marshall Brown, Gabrielle Alonzi, Mersine A Bryan, Cordelia Burn, Joyce C Chang, Jonathan D Cogen, Nidhi Naik, Kareena Patel, Emily Zhang, Esi M Morgan, MaryBeth Son","doi":"10.1136/lupus-2025-001607","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Youth with childhood-onset SLE (cSLE) have increased risk of serious infection. It is unknown how much of this risk is due to modifiable factors such as choice of immunosuppressant. We aimed to compare hospitalised infection rates in youth with cSLE on different disease-modifying antirheumatic drugs (DMARDs).</p><p><strong>Methods: </strong>We included youth ≤18 years with cSLE treated from 2009 to 2022 at two centres. Clinical data were extracted from electronic health records and the Paediatric Health Information System. Hospitalised infection frequency was calculated over the first year of treatment in youth included in each DMARD exposure group, stratified by lupus nephritis (LN) status. Cox proportional hazard regression with inverse probability of treatment weighting (IPTW) was used to compare infection rates across DMARD groups, adjusting for corticosteroid dose.</p><p><strong>Results: </strong>Among 257 youths with cSLE, 5% had ≥1 hospitalised infection within 1 year of DMARD initiation. 8% of those with LN had ≥1 hospitalised infection compared with 2.5% without LN. In IPTW-adjusted models, children with LN treated with mycophenolate had lower risk of infection compared with those treated with cyclophosphamide (HR 0.12; 95% CI 0.019 to 0.88). Among those without LN, mycophenolate did not differ from azathioprine in infection risk (HR 1.67, 95% CI 0.56 to 4.99). Higher oral corticosteroid dosing (per 1 mg/day of prednisone) was associated with increased risk of infection (HR 1.1, 95% CI 1.05 to 1.15).</p><p><strong>Conclusions: </strong>We observed higher hospitalised infection rates in children with cSLE and LN compared with those without LN. Among children with LN, those who received cyclophosphamide had more infections than those who received mycophenolate. Methotrexate was associated with lower infection rates than mycophenolate or azathioprine among youth without LN. Higher daily oral steroid dose was significantly associated with increased hospitalised infection risk in youth with non-renal SLE.</p>","PeriodicalId":18126,"journal":{"name":"Lupus Science & Medicine","volume":"12 2","pages":""},"PeriodicalIF":3.5000,"publicationDate":"2025-09-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12458716/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lupus Science & Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/lupus-2025-001607","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Youth with childhood-onset SLE (cSLE) have increased risk of serious infection. It is unknown how much of this risk is due to modifiable factors such as choice of immunosuppressant. We aimed to compare hospitalised infection rates in youth with cSLE on different disease-modifying antirheumatic drugs (DMARDs).
Methods: We included youth ≤18 years with cSLE treated from 2009 to 2022 at two centres. Clinical data were extracted from electronic health records and the Paediatric Health Information System. Hospitalised infection frequency was calculated over the first year of treatment in youth included in each DMARD exposure group, stratified by lupus nephritis (LN) status. Cox proportional hazard regression with inverse probability of treatment weighting (IPTW) was used to compare infection rates across DMARD groups, adjusting for corticosteroid dose.
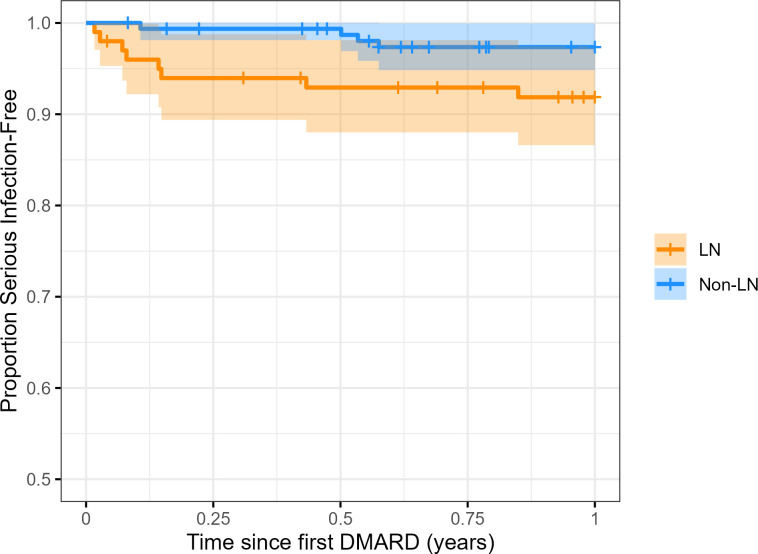
Results: Among 257 youths with cSLE, 5% had ≥1 hospitalised infection within 1 year of DMARD initiation. 8% of those with LN had ≥1 hospitalised infection compared with 2.5% without LN. In IPTW-adjusted models, children with LN treated with mycophenolate had lower risk of infection compared with those treated with cyclophosphamide (HR 0.12; 95% CI 0.019 to 0.88). Among those without LN, mycophenolate did not differ from azathioprine in infection risk (HR 1.67, 95% CI 0.56 to 4.99). Higher oral corticosteroid dosing (per 1 mg/day of prednisone) was associated with increased risk of infection (HR 1.1, 95% CI 1.05 to 1.15).
Conclusions: We observed higher hospitalised infection rates in children with cSLE and LN compared with those without LN. Among children with LN, those who received cyclophosphamide had more infections than those who received mycophenolate. Methotrexate was associated with lower infection rates than mycophenolate or azathioprine among youth without LN. Higher daily oral steroid dose was significantly associated with increased hospitalised infection risk in youth with non-renal SLE.
期刊介绍:
Lupus Science & Medicine is a global, peer reviewed, open access online journal that provides a central point for publication of basic, clinical, translational, and epidemiological studies of all aspects of lupus and related diseases. It is the first lupus-specific open access journal in the world and was developed in response to the need for a barrier-free forum for publication of groundbreaking studies in lupus. The journal publishes research on lupus from fields including, but not limited to: rheumatology, dermatology, nephrology, immunology, pediatrics, cardiology, hepatology, pulmonology, obstetrics and gynecology, and psychiatry.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


