Christian Maalouli, Selda Aydin, Alix Collard, Jean-Francois Cambier, Agnes Dejardin, Benoit Georges, Gaelle Gillerot, Benedicte Vanderperren, Ann-Karolien Vandooren, Michel Jadoul, Johann Morelle, Nathalie Demoulin
{"title":"Predicting prognosis in ANCA-associated vasculitis with kidney involvement.","authors":"Christian Maalouli, Selda Aydin, Alix Collard, Jean-Francois Cambier, Agnes Dejardin, Benoit Georges, Gaelle Gillerot, Benedicte Vanderperren, Ann-Karolien Vandooren, Michel Jadoul, Johann Morelle, Nathalie Demoulin","doi":"10.1093/ckj/sfaf268","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The ANCA Renal Risk Score was updated in 2023 to the ANCA Kidney Risk Score (AKRiS) to improve clinicopathological prognostication in patients with anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) and kidney involvement. Our study aimed to assess whether incorporating recently identified predictors of kidney survival in AAV could further refine the prognostic accuracy of AKRiS in our multicentric cohort.</p><p><strong>Methods: </strong>We retrospectively reviewed all incident AAV with kidney biopsy from 2005 to 2020. Cox regression analysis examined factors [AKRiS, dialysis within 4 weeks, urine protein-creatinine ratio (UPCR) and hematuria at baseline, C3 deposits, renal arteritis on biopsy, estimated glomerular filtration rate (eGFR), UPCR and hematuria after induction] associated with kidney failure. These factors in combination with AKRiS were analyzed using the area under the receiver operating characteristic curve (AUROC) for prediction of kidney failure.</p><p><strong>Results: </strong>The cohort included 115 patients (age 64 years, 55% male, 57% myeloperoxidase-ANCA, baseline creatinine 3.6 mg/dL, eGFR 16 mL/min/1.73 m<sup>2</sup>), with 34 (30%) dialysed within 4 weeks. During a median 6.4-year follow-up, 39 (34%) patients progressed to kidney failure, and 13 (11%) died. Cox analysis identified AKRiS, dialysis within 4 weeks, C3 deposits, renal arteritis on biopsy, lower eGFR after induction and higher UPCR after induction as unadjusted risk factors for kidney failure. After adjusting for AKRiS, dialysis within 4 weeks [hazard ratio (HR) 6.20 (95% confidence interval 2.76 to 13.95), <i>P</i> ≤ .001], eGFR after induction [HR 0.94 (0.89 to 0.99), <i>P </i>= .03] and UPCR after induction [HR 1.62 (1.02 to 2.58), <i>P </i>= .04] remained significantly associated with kidney outcome. The AUROC for kidney failure prediction was 0.77 for AKRiS, increasing to 0.82, 0.80 and 0.79 when adding dialysis within 4 weeks, eGFR and UPCR after induction, respectively.</p><p><strong>Conclusion: </strong>Dialysis within 4 weeks, eGFR after induction and UPCR after induction are able to predict long-term kidney outcome in AAV patients. Adjusting AKRiS for these variables modestly enhances its predictive power. We propose using them as placeholder endpoints for kidney failure in future studies.</p>","PeriodicalId":10435,"journal":{"name":"Clinical Kidney Journal","volume":"18 9","pages":"sfaf268"},"PeriodicalIF":4.6000,"publicationDate":"2025-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12451443/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Kidney Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ckj/sfaf268","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The ANCA Renal Risk Score was updated in 2023 to the ANCA Kidney Risk Score (AKRiS) to improve clinicopathological prognostication in patients with anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) and kidney involvement. Our study aimed to assess whether incorporating recently identified predictors of kidney survival in AAV could further refine the prognostic accuracy of AKRiS in our multicentric cohort.
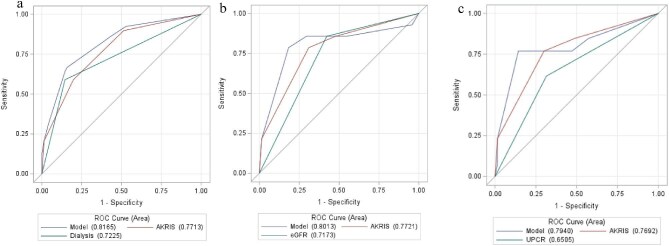
Methods: We retrospectively reviewed all incident AAV with kidney biopsy from 2005 to 2020. Cox regression analysis examined factors [AKRiS, dialysis within 4 weeks, urine protein-creatinine ratio (UPCR) and hematuria at baseline, C3 deposits, renal arteritis on biopsy, estimated glomerular filtration rate (eGFR), UPCR and hematuria after induction] associated with kidney failure. These factors in combination with AKRiS were analyzed using the area under the receiver operating characteristic curve (AUROC) for prediction of kidney failure.
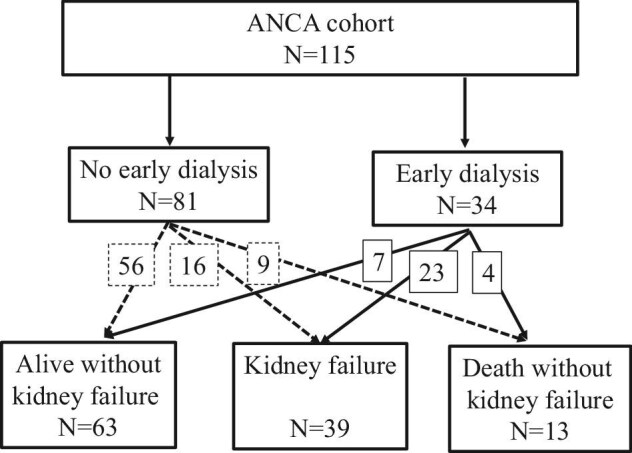
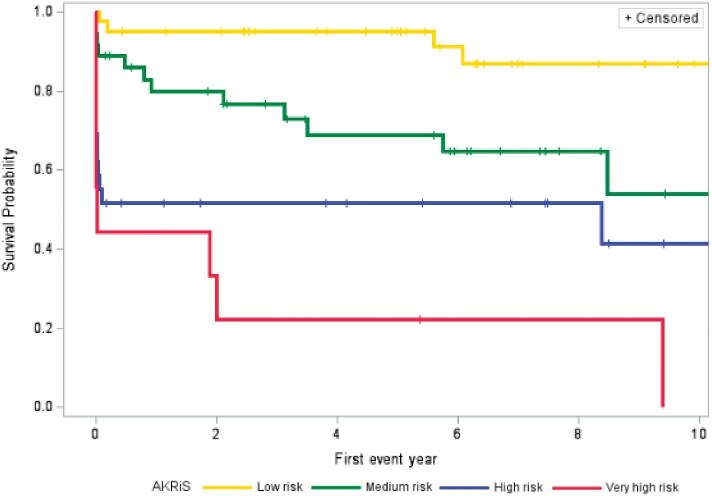
Results: The cohort included 115 patients (age 64 years, 55% male, 57% myeloperoxidase-ANCA, baseline creatinine 3.6 mg/dL, eGFR 16 mL/min/1.73 m2), with 34 (30%) dialysed within 4 weeks. During a median 6.4-year follow-up, 39 (34%) patients progressed to kidney failure, and 13 (11%) died. Cox analysis identified AKRiS, dialysis within 4 weeks, C3 deposits, renal arteritis on biopsy, lower eGFR after induction and higher UPCR after induction as unadjusted risk factors for kidney failure. After adjusting for AKRiS, dialysis within 4 weeks [hazard ratio (HR) 6.20 (95% confidence interval 2.76 to 13.95), P ≤ .001], eGFR after induction [HR 0.94 (0.89 to 0.99), P = .03] and UPCR after induction [HR 1.62 (1.02 to 2.58), P = .04] remained significantly associated with kidney outcome. The AUROC for kidney failure prediction was 0.77 for AKRiS, increasing to 0.82, 0.80 and 0.79 when adding dialysis within 4 weeks, eGFR and UPCR after induction, respectively.
Conclusion: Dialysis within 4 weeks, eGFR after induction and UPCR after induction are able to predict long-term kidney outcome in AAV patients. Adjusting AKRiS for these variables modestly enhances its predictive power. We propose using them as placeholder endpoints for kidney failure in future studies.
期刊介绍:
About the Journal
Clinical Kidney Journal: Clinical and Translational Nephrology (ckj), an official journal of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association), is a fully open access, online only journal publishing bimonthly. The journal is an essential educational and training resource integrating clinical, translational and educational research into clinical practice. ckj aims to contribute to a translational research culture among nephrologists and kidney pathologists that helps close the gap between basic researchers and practicing clinicians and promote sorely needed innovation in the Nephrology field. All research articles in this journal have undergone peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


