The incidence of coronary in-stent restenosis and the rate of reaching the standard of low-density lipoprotein cholesterol in patients with type 2 diabetes mellitus and unstable angina pectoris treated with ezetimibe and rosuvastatin.
{"title":"The incidence of coronary in-stent restenosis and the rate of reaching the standard of low-density lipoprotein cholesterol in patients with type 2 diabetes mellitus and unstable angina pectoris treated with ezetimibe and rosuvastatin.","authors":"Fanhao Ye, Hao Chen, Hebo Li","doi":"10.3389/fcvm.2025.1599313","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Diabetes is closely associated with the occurrence and development of coronary atherosclerotic heart disease. Coronary atherosclerosis is often severe and diffuse in patients with diabetes. We investigated the incidence of coronary in-stent restenosis (ISR) and the rate of reaching the standard of low-density lipoprotein cholesterol (LDL-C) in patients with type 2 diabetes mellitus (T2DM) and unstable angina pectoris (UAP) treated with ezetimibe and rosuvastatin one year later.</p><p><strong>Materials and methods: </strong>We selected the first pair of UAP patients with T2DM who underwent coronary artery stent implantation at our hospital between October 2018 and February 2022. According to drug use, the patients were divided into the rosuvastatin group [61 cases, rosuvastatin 10 mg/qn (every night)] and the combined group [60 cases, ezetimibe 10 mg/qd (once daily) and rosuvastatin 10 mg/qn]. Biochemical indices, left ventricular ejection fraction, and left ventricular end-diastolic diameter were collected before and one year after the first percutaneous coronary intervention. We collected data on the incidence of ISR and the rate of reaching the standard of LDL-C one year after surgery. Emergency PCI or coronary artery bypass grafting, cardiac death, and non-fatal acute myocardial infarction due to unstable angina pectoris 30 days after coronary stent implantation and lipid-lowering treatment were regarded as the primary endpoints.</p><p><strong>Results: </strong>After one year of follow-up, the incidence of in-stent restenosis(ISR), total cholesterol(TC), and LDL-C levels in the combined group[ISR, 3.33%; TC, 3.19 ± 0.75; LDL-C, 1.38(1.18-1.64)] were lower than those in the rosuvastatin group[ISR, 16.39% TC,C 3.84 ± 1.15; LDL-C, 1.92(1.52-2.61)] (<i>P</i> < 0.05). The rate of reaching the standard of LDL-C in the combined group (65%, 95% CI 0.560-0.809) was higher than that in the rosuvastatin group(31%, 95% CI 0.210-0.446) (<i>P</i> < 0.05). No significant difference in safety was observed between the two groups (<i>P</i> > 0.05). No endpoints were observed in the combined group.</p><p><strong>Conclusion: </strong>Resuvastatin combined with ezetimibe can better prevent ISR and reduce the incidence of cardiovascular adverse events. In addition, ezetimibe combined with rosuvastatin better reduced LDL-C levels.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"12 ","pages":"1599313"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12451000/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2025.1599313","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Diabetes is closely associated with the occurrence and development of coronary atherosclerotic heart disease. Coronary atherosclerosis is often severe and diffuse in patients with diabetes. We investigated the incidence of coronary in-stent restenosis (ISR) and the rate of reaching the standard of low-density lipoprotein cholesterol (LDL-C) in patients with type 2 diabetes mellitus (T2DM) and unstable angina pectoris (UAP) treated with ezetimibe and rosuvastatin one year later.
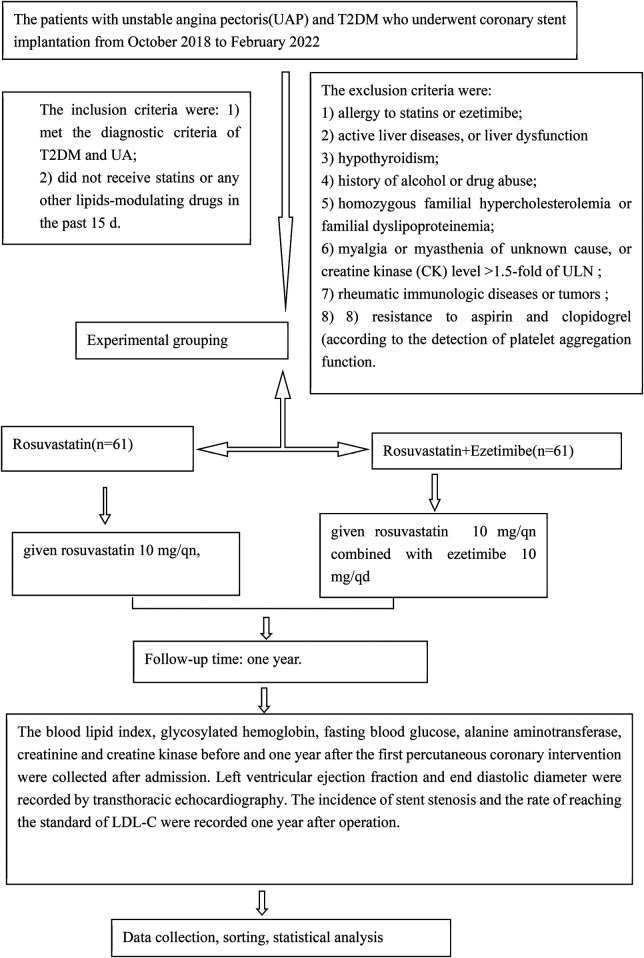
Materials and methods: We selected the first pair of UAP patients with T2DM who underwent coronary artery stent implantation at our hospital between October 2018 and February 2022. According to drug use, the patients were divided into the rosuvastatin group [61 cases, rosuvastatin 10 mg/qn (every night)] and the combined group [60 cases, ezetimibe 10 mg/qd (once daily) and rosuvastatin 10 mg/qn]. Biochemical indices, left ventricular ejection fraction, and left ventricular end-diastolic diameter were collected before and one year after the first percutaneous coronary intervention. We collected data on the incidence of ISR and the rate of reaching the standard of LDL-C one year after surgery. Emergency PCI or coronary artery bypass grafting, cardiac death, and non-fatal acute myocardial infarction due to unstable angina pectoris 30 days after coronary stent implantation and lipid-lowering treatment were regarded as the primary endpoints.
Results: After one year of follow-up, the incidence of in-stent restenosis(ISR), total cholesterol(TC), and LDL-C levels in the combined group[ISR, 3.33%; TC, 3.19 ± 0.75; LDL-C, 1.38(1.18-1.64)] were lower than those in the rosuvastatin group[ISR, 16.39% TC,C 3.84 ± 1.15; LDL-C, 1.92(1.52-2.61)] (P < 0.05). The rate of reaching the standard of LDL-C in the combined group (65%, 95% CI 0.560-0.809) was higher than that in the rosuvastatin group(31%, 95% CI 0.210-0.446) (P < 0.05). No significant difference in safety was observed between the two groups (P > 0.05). No endpoints were observed in the combined group.
Conclusion: Resuvastatin combined with ezetimibe can better prevent ISR and reduce the incidence of cardiovascular adverse events. In addition, ezetimibe combined with rosuvastatin better reduced LDL-C levels.
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


