Niels A Stens, Geert A A Versteeg, Maxim J P Rooijakkers, Roos de Lange, Stijn J H Bonekamp, Marleen H van Wely, Robert Jan M van Geuns, Michel W A Verkroost, Leen A F M van Garsse, Guillaume S C Geuzebroek, Robin H Heijmen, Lokien X van Nunen, Dick H J Thijssen, Niels van Royen
{"title":"Construct validity of automated assessment of invasively measured hemodynamics during transcatheter aortic valve replacement.","authors":"Niels A Stens, Geert A A Versteeg, Maxim J P Rooijakkers, Roos de Lange, Stijn J H Bonekamp, Marleen H van Wely, Robert Jan M van Geuns, Michel W A Verkroost, Leen A F M van Garsse, Guillaume S C Geuzebroek, Robin H Heijmen, Lokien X van Nunen, Dick H J Thijssen, Niels van Royen","doi":"10.1093/ehjdh/ztaf069","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Paravalvular regurgitation (PVR) is frequently observed following Transcatheter Aortic Valve Replacement (TAVR). Periprocedural monitoring of invasive hemodynamics has shown promise for diagnosis of PVR, but automated software options are lacking. We aimed to develop a rule-based algorithm for automated assessment of hemodynamic indices of PVR, and evaluate its construct validity and discriminatory value for cardiac magnetic resonance (CMR)-derived relevant PVR compared to standard manual hemodynamic assessment.</p><p><strong>Methods and results: </strong>Left ventricular and aortic pressures were invasively measured during TAVR using fluid-filled pigtail catheters. To evaluate construct validity of automated vs. manual assessment of invasive hemodynamics, we compared (i) proportion of cardiac cycles affected by arrhythmias/noise, (ii) pressure gradients, and (iii) PVR indices. Additionally, we compared the discriminatory value of automatically and manually determined PVR indices for CMR-determined relevant PVR at 30-days. In total, 77 patients were enrolled (664 cardiac cycles). Automated filtering of cardiac cycles affected by arrhythmias/noise had a high sensitivity (95.2%) and specificity (86.4%). In addition, excellent agreement was observed between automated and manual computation of mean gradients pre- and post-TAVR [39.3 ± 12.1 vs. 37.5 ± 11.9 mmHg, intra-class correlation coefficient (ICC): 0.916; 1.92 ± 5.87 vs. 1.14 ± 5.89, ICC: 0.957, respectively], and PVR indices [diastolic delta (DD): 41.7 ± 12.4 vs. 40.6 ± 12.3 mmHg, ICC: 0.982, respectively]. Automated and manual assessment of DD showed comparable discriminatory value for relevant PVR [area under the curve (AUC): 0.81 vs. 0.80, respectively].</p><p><strong>Conclusion: </strong>Rule-based, automated assessment of hemodynamic indices of PVR showed excellent construct validity and discriminatory value for CMR-determined relevant PVR, supporting its use for real-time evaluation and risk stratification in TAVR patients.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"6 5","pages":"1006-1014"},"PeriodicalIF":4.4000,"publicationDate":"2025-06-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12450506/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztaf069","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Paravalvular regurgitation (PVR) is frequently observed following Transcatheter Aortic Valve Replacement (TAVR). Periprocedural monitoring of invasive hemodynamics has shown promise for diagnosis of PVR, but automated software options are lacking. We aimed to develop a rule-based algorithm for automated assessment of hemodynamic indices of PVR, and evaluate its construct validity and discriminatory value for cardiac magnetic resonance (CMR)-derived relevant PVR compared to standard manual hemodynamic assessment.
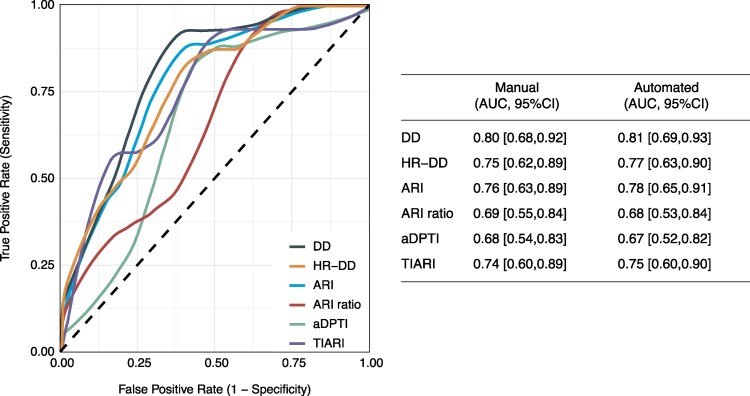
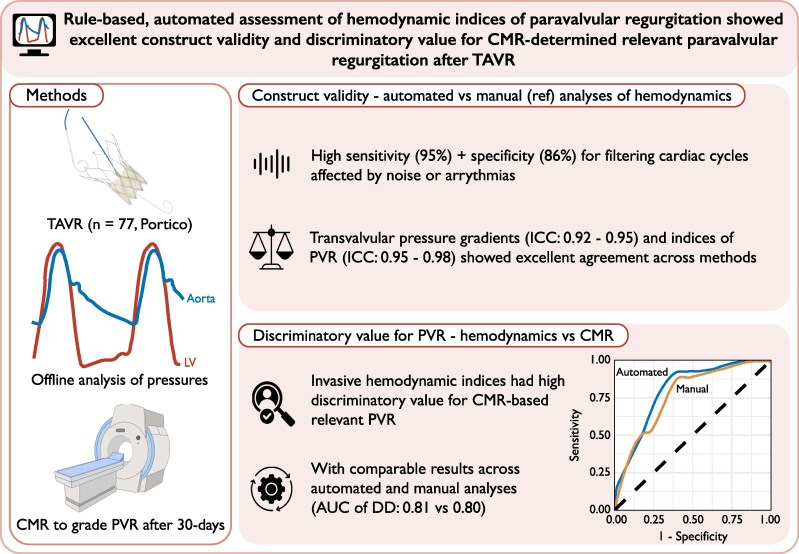
Methods and results: Left ventricular and aortic pressures were invasively measured during TAVR using fluid-filled pigtail catheters. To evaluate construct validity of automated vs. manual assessment of invasive hemodynamics, we compared (i) proportion of cardiac cycles affected by arrhythmias/noise, (ii) pressure gradients, and (iii) PVR indices. Additionally, we compared the discriminatory value of automatically and manually determined PVR indices for CMR-determined relevant PVR at 30-days. In total, 77 patients were enrolled (664 cardiac cycles). Automated filtering of cardiac cycles affected by arrhythmias/noise had a high sensitivity (95.2%) and specificity (86.4%). In addition, excellent agreement was observed between automated and manual computation of mean gradients pre- and post-TAVR [39.3 ± 12.1 vs. 37.5 ± 11.9 mmHg, intra-class correlation coefficient (ICC): 0.916; 1.92 ± 5.87 vs. 1.14 ± 5.89, ICC: 0.957, respectively], and PVR indices [diastolic delta (DD): 41.7 ± 12.4 vs. 40.6 ± 12.3 mmHg, ICC: 0.982, respectively]. Automated and manual assessment of DD showed comparable discriminatory value for relevant PVR [area under the curve (AUC): 0.81 vs. 0.80, respectively].
Conclusion: Rule-based, automated assessment of hemodynamic indices of PVR showed excellent construct validity and discriminatory value for CMR-determined relevant PVR, supporting its use for real-time evaluation and risk stratification in TAVR patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


