Evaluation of machine learning models for personalized prediction of benefit from temporary mechanical circulatory support after out-of-hospital cardiac arrest.
Julian Kreutz, Jonathan Bamberger, Lukas Harbaum, Klevis Mihali, Georgios Chatzis, Nikolaos Patsalis, Mohamed Ben Amar, Styliani Syntila, Martin C Hirsch, Fabian Lechner, Bernhard Schieffer, Birgit Markus
{"title":"Evaluation of machine learning models for personalized prediction of benefit from temporary mechanical circulatory support after out-of-hospital cardiac arrest.","authors":"Julian Kreutz, Jonathan Bamberger, Lukas Harbaum, Klevis Mihali, Georgios Chatzis, Nikolaos Patsalis, Mohamed Ben Amar, Styliani Syntila, Martin C Hirsch, Fabian Lechner, Bernhard Schieffer, Birgit Markus","doi":"10.1093/ehjdh/ztaf082","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The role of temporary mechanical circulatory support (tMCS) after out-of-hospital cardiac arrest (OHCA) remains controversial. This study evaluates machine learning (ML) models for predicting mortality and neurological outcomes, highlighting their potential as a tool to guide early tMCS decision-making.</p><p><strong>Methods and results: </strong>This retrospective study analysed five years of data from 564 adult non-traumatic OHCA patients treated at Marburg University Hospital. Four ML models (ANN, SVM, RF, XGBoost) were trained to predict in-hospital mortality and neurological outcome based on demographic, clinical, and treatment-related variables. Feature selection and SHAP analysis were used to optimize performance and identify patients potentially benefiting from tMCS. Overall, 144 patients (31.2%) out of 461 patients who fulfilled the inclusion criteria received tMCS: 39 left-ventricular microaxial flow pump, 76 venoarterial extracorporeal membrane oxygenation (VA-ECMO), and 29 biventricular support (ECMELLA). In 69 patients (14.9%) VA-ECMO implantation was performed as part of extracorporeal cardiopulmonary resuscitation. The survival rate of the tMCS group was 34.7% (50/144) compared to 52.7% (167/317) in the non-tMCS group. The highest predictive power for survival probability (with/without tMCS) could be achieved by XGBoost and RF when applied to the non-tMCS group. Machine learning identified 2.5% of non-tMCS patients likely to survive if treated with tMCS. In 23 (RF model) and 31 (XGBoost model) patients, the probability of survival increased by at least 5% with tMCS compared to their predicted outcome without tMCS. RF slightly outperformed XGBoost [area under the receiver operating characteristic curve (AUC) 0.85 vs. AUC 0.82].</p><p><strong>Conclusion: </strong>XGBoost and RF models accurately predict mortality and tMCS benefit in OHCA patients, supporting ML-based personalized therapy.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"6 5","pages":"979-988"},"PeriodicalIF":4.4000,"publicationDate":"2025-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12450520/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztaf082","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: The role of temporary mechanical circulatory support (tMCS) after out-of-hospital cardiac arrest (OHCA) remains controversial. This study evaluates machine learning (ML) models for predicting mortality and neurological outcomes, highlighting their potential as a tool to guide early tMCS decision-making.
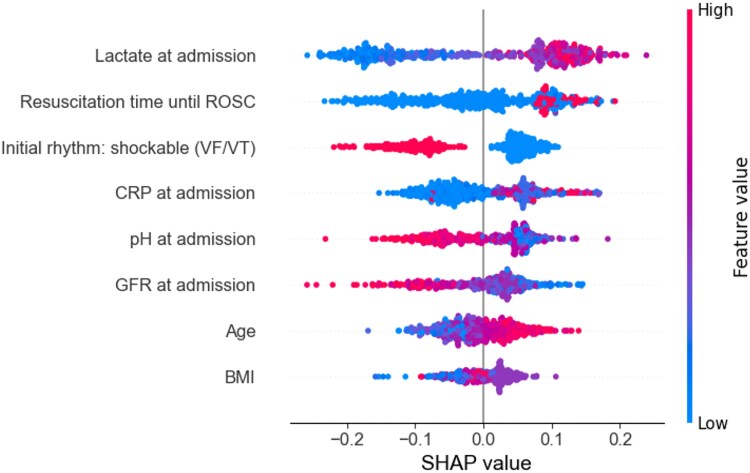
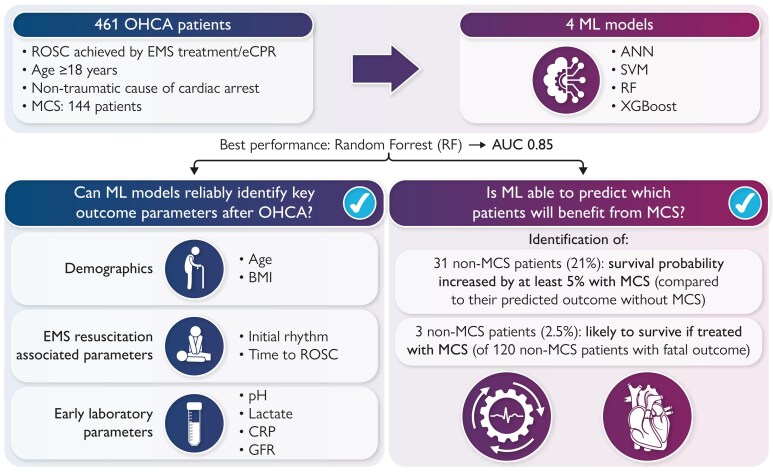
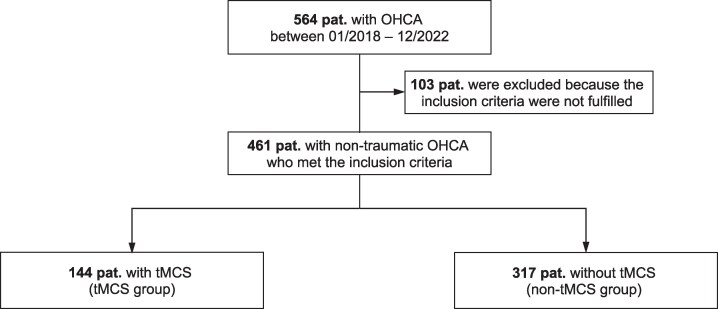
Methods and results: This retrospective study analysed five years of data from 564 adult non-traumatic OHCA patients treated at Marburg University Hospital. Four ML models (ANN, SVM, RF, XGBoost) were trained to predict in-hospital mortality and neurological outcome based on demographic, clinical, and treatment-related variables. Feature selection and SHAP analysis were used to optimize performance and identify patients potentially benefiting from tMCS. Overall, 144 patients (31.2%) out of 461 patients who fulfilled the inclusion criteria received tMCS: 39 left-ventricular microaxial flow pump, 76 venoarterial extracorporeal membrane oxygenation (VA-ECMO), and 29 biventricular support (ECMELLA). In 69 patients (14.9%) VA-ECMO implantation was performed as part of extracorporeal cardiopulmonary resuscitation. The survival rate of the tMCS group was 34.7% (50/144) compared to 52.7% (167/317) in the non-tMCS group. The highest predictive power for survival probability (with/without tMCS) could be achieved by XGBoost and RF when applied to the non-tMCS group. Machine learning identified 2.5% of non-tMCS patients likely to survive if treated with tMCS. In 23 (RF model) and 31 (XGBoost model) patients, the probability of survival increased by at least 5% with tMCS compared to their predicted outcome without tMCS. RF slightly outperformed XGBoost [area under the receiver operating characteristic curve (AUC) 0.85 vs. AUC 0.82].
Conclusion: XGBoost and RF models accurately predict mortality and tMCS benefit in OHCA patients, supporting ML-based personalized therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


