Ali Saad Alshahrani, Yazan Jumah Alalwani, Nihal Mushabb Alqahtani, Abdullah Shafi D Alanazi, Ahmed Khaled Almarri, Shatha Saud Alqurashi, Deemah Khalid Ghazi, Abdullah Musaaed Alsalamah, Rahaf Hamdan Alruwaili, Ahmed Y Azzam, Fawaz Alanii
{"title":"Outcomes of autologous bone grafts <i>vs</i> bone substitutes in tibial plateau fractures: A meta-analysis.","authors":"Ali Saad Alshahrani, Yazan Jumah Alalwani, Nihal Mushabb Alqahtani, Abdullah Shafi D Alanazi, Ahmed Khaled Almarri, Shatha Saud Alqurashi, Deemah Khalid Ghazi, Abdullah Musaaed Alsalamah, Rahaf Hamdan Alruwaili, Ahmed Y Azzam, Fawaz Alanii","doi":"10.5312/wjo.v16.i9.111068","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Tibial plateau fractures often require structural support for metaphyseal defects created during articular reduction. While autologous bone grafting has been utilized as the gold standard, bone substitutes offer advantages including reduced donor site morbidity. Our meta-analysis evaluated the comparative efficacy of these approaches across clinical and operative outcomes.</p><p><strong>Aim: </strong>To conduct a systematic review and meta-analysis of randomized controlled trials comparing autologous bone grafts with bone substitutes for tibial plateau fractures.</p><p><strong>Methods: </strong>We conducted a systematic review and meta-analysis of randomized controlled trials comparing autologous bone grafts with bone substitutes for tibial plateau fractures. Primary outcomes included joint depression, secondary collapse rate, operative time, blood loss, and infection rate. Subgroup analyses were performed by fracture complexity, geographic region, and methodological factors. In addition to that, we also developed a combined outcome score integrating structural, procedural, and complication domains.</p><p><strong>Results: </strong>Seven randomized controlled trials with 424 patients (296 bone substitute, 128 autograft) were included. No significant differences in joint depression or secondary collapse were observed across fracture complexity categories. Geographic variations were evident, with Western studies showing significantly higher risk of secondary collapse with autografts (risk ratio = 1.45, <i>P</i> value = 0.02). Both Western and Asian studies have demonstrated significantly reduced blood loss with bone substitutes (70-90 mL less), while operative time reduction was more significant in the Asian studies (23.65 <i>vs</i> 8.00 minutes, <i>P</i> value = 0.04 for subgroup difference). The combined outcome score (standardized effect size -0.2481) favored bone substitutes, primarily due to procedural advantages.</p><p><strong>Conclusion: </strong>Bone substitutes provide similar structural outcomes to autologous bone grafts while having better procedural advantages in tibial plateau fracture management. These findings support bone substitutes as a viable option across fracture patterns. Future studies should focus on specific bone substitute formulations and cost-effectiveness analyses.</p>","PeriodicalId":47843,"journal":{"name":"World Journal of Orthopedics","volume":"16 9","pages":"111068"},"PeriodicalIF":2.3000,"publicationDate":"2025-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12444308/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Orthopedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5312/wjo.v16.i9.111068","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Tibial plateau fractures often require structural support for metaphyseal defects created during articular reduction. While autologous bone grafting has been utilized as the gold standard, bone substitutes offer advantages including reduced donor site morbidity. Our meta-analysis evaluated the comparative efficacy of these approaches across clinical and operative outcomes.
Aim: To conduct a systematic review and meta-analysis of randomized controlled trials comparing autologous bone grafts with bone substitutes for tibial plateau fractures.
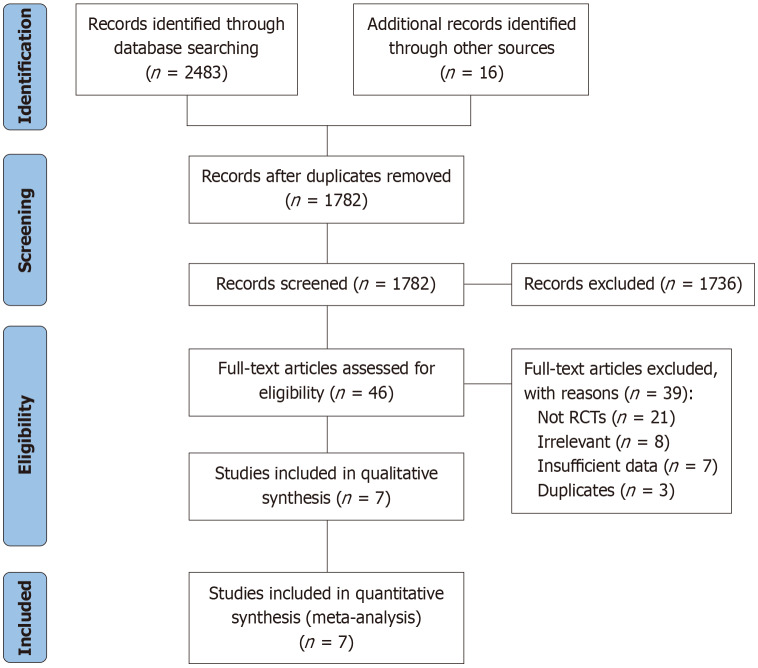
Methods: We conducted a systematic review and meta-analysis of randomized controlled trials comparing autologous bone grafts with bone substitutes for tibial plateau fractures. Primary outcomes included joint depression, secondary collapse rate, operative time, blood loss, and infection rate. Subgroup analyses were performed by fracture complexity, geographic region, and methodological factors. In addition to that, we also developed a combined outcome score integrating structural, procedural, and complication domains.
Results: Seven randomized controlled trials with 424 patients (296 bone substitute, 128 autograft) were included. No significant differences in joint depression or secondary collapse were observed across fracture complexity categories. Geographic variations were evident, with Western studies showing significantly higher risk of secondary collapse with autografts (risk ratio = 1.45, P value = 0.02). Both Western and Asian studies have demonstrated significantly reduced blood loss with bone substitutes (70-90 mL less), while operative time reduction was more significant in the Asian studies (23.65 vs 8.00 minutes, P value = 0.04 for subgroup difference). The combined outcome score (standardized effect size -0.2481) favored bone substitutes, primarily due to procedural advantages.
Conclusion: Bone substitutes provide similar structural outcomes to autologous bone grafts while having better procedural advantages in tibial plateau fracture management. These findings support bone substitutes as a viable option across fracture patterns. Future studies should focus on specific bone substitute formulations and cost-effectiveness analyses.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


