{"title":"Fractional excretion of sodium and 1-year cardiovascular mortality in acute decompensated heart failure, is there any relationship?","authors":"Seyed Hossein Sharoubandi, Maryam Moshkani Farahani, Arezoo Khosravi, Najmeh Rabanipour","doi":"10.4103/jrms.jrms_153_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Renal impairment (RI), the most common comorbidity in acute decompensated heart failure (ADHF) patients, leads to cardiorenal syndrome. Fractional excretion of sodium (FENa), an indicator of sodium handling by the kidney, is widely used to assess natriuresis, the underlying treatment of ADHF. The aim of this study was to investigate the association of FENa with RI and 1-year cardiovascular mortality.</p><p><strong>Materials and methods: </strong>This prospective study was implemented in the Persian Registry of Cardiovascular Disease/Heart Failure study context. Any individuals over 18 years suffering from ADHF admitted to the emergency department were eligible to be recruited in our study. We excluded the patients with previously untreated chronic comorbidities, who died during hospitalization, and without follow-up and other etiologies rather than cardiovascular diseases since discharge. Baseline demographic and clinical data gathered. RI was defined as a 0.3 mg/dL rise of creatinine during admission. The primary and secondary clinical outcomes were RI and cardiovascular mortality, respectively.</p><p><strong>Results: </strong>During the study period, 158 patients were recruited, with 103 (65.1%) developing RI and 25.68% of the population expired. Higher blood pressure, overall furosemide dose, as well as lower FENa, and serum creatinine on admission were prevalent among patients who developed RI. Greater serum sodium levels on admission and discharge, a lack of a history of ischemic heart disease, and hyponatremic status during admission were associated with a higher mortality rate. The Pearson correlations demonstrate the significant association of FENa with creatinine alterations (<i>P</i> = 0.001, <i>r</i> = -0.47). The linear regression analysis demonstrates the significant association of FENa with creatinine alteration during admission (<i>B</i> = -1.43, 95% confidence interval [CI] [- 1.86, -1.002], <i>P</i> = 0.001). Multiple logistic regression demonstrates no significant association of prediction of FENa with creatinine alterations (odds ratio [OR] =0.33, 95% CI [0.09-1.19], <i>P</i> = 0.091). The logistic regression analysis revealed no association between FENa and 1-year mortality (OR = 0.85, 95% CI (0.26-2.75), <i>P</i> = 0.79).</p><p><strong>Conclusion: </strong>A lower FENa on admission indirectly predicts the development of RI in patients with ADHF. Meanwhile, FENa is unable to predict 1-year cardiovascular mortality.</p>","PeriodicalId":50062,"journal":{"name":"Journal of Research in Medical Sciences","volume":"30 ","pages":"41"},"PeriodicalIF":1.5000,"publicationDate":"2025-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12445762/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Research in Medical Sciences","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4103/jrms.jrms_153_23","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Renal impairment (RI), the most common comorbidity in acute decompensated heart failure (ADHF) patients, leads to cardiorenal syndrome. Fractional excretion of sodium (FENa), an indicator of sodium handling by the kidney, is widely used to assess natriuresis, the underlying treatment of ADHF. The aim of this study was to investigate the association of FENa with RI and 1-year cardiovascular mortality.
Materials and methods: This prospective study was implemented in the Persian Registry of Cardiovascular Disease/Heart Failure study context. Any individuals over 18 years suffering from ADHF admitted to the emergency department were eligible to be recruited in our study. We excluded the patients with previously untreated chronic comorbidities, who died during hospitalization, and without follow-up and other etiologies rather than cardiovascular diseases since discharge. Baseline demographic and clinical data gathered. RI was defined as a 0.3 mg/dL rise of creatinine during admission. The primary and secondary clinical outcomes were RI and cardiovascular mortality, respectively.
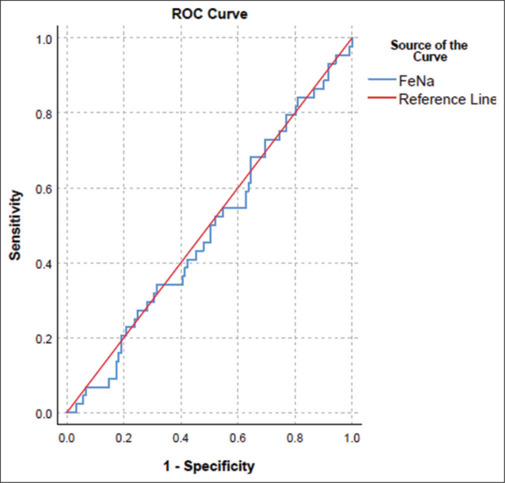
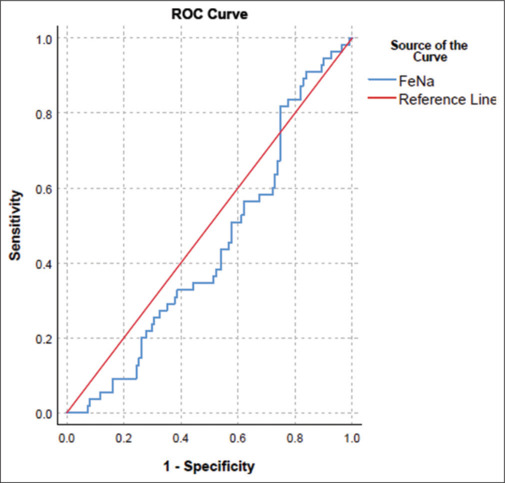
Results: During the study period, 158 patients were recruited, with 103 (65.1%) developing RI and 25.68% of the population expired. Higher blood pressure, overall furosemide dose, as well as lower FENa, and serum creatinine on admission were prevalent among patients who developed RI. Greater serum sodium levels on admission and discharge, a lack of a history of ischemic heart disease, and hyponatremic status during admission were associated with a higher mortality rate. The Pearson correlations demonstrate the significant association of FENa with creatinine alterations (P = 0.001, r = -0.47). The linear regression analysis demonstrates the significant association of FENa with creatinine alteration during admission (B = -1.43, 95% confidence interval [CI] [- 1.86, -1.002], P = 0.001). Multiple logistic regression demonstrates no significant association of prediction of FENa with creatinine alterations (odds ratio [OR] =0.33, 95% CI [0.09-1.19], P = 0.091). The logistic regression analysis revealed no association between FENa and 1-year mortality (OR = 0.85, 95% CI (0.26-2.75), P = 0.79).
Conclusion: A lower FENa on admission indirectly predicts the development of RI in patients with ADHF. Meanwhile, FENa is unable to predict 1-year cardiovascular mortality.
期刊介绍:
Journal of Research in Medical Sciences, a publication of Isfahan University of Medical Sciences, is a peer-reviewed online continuous journal with print on demand compilation of issues published. The journal’s full text is available online at http://www.jmsjournal.net. The journal allows free access (Open Access) to its contents and permits authors to self-archive final accepted version of the articles on any OAI-compliant institutional / subject-based repository.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


