Omar Lubbad, Wajeeh Ullah Mahmood, Shehram Shafique, Krishna K Singh, Goldie Khera, Muhammad Shafique Sajid
{"title":"Effect of prehabilitation in patients undergoing gastric or oesophageal cancer resections: A systematic review and meta-analysis.","authors":"Omar Lubbad, Wajeeh Ullah Mahmood, Shehram Shafique, Krishna K Singh, Goldie Khera, Muhammad Shafique Sajid","doi":"10.4253/wjge.v17.i9.109033","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Gastric and oesophageal cancers are among the leading causes of cancer-related mortality globally. Treatment in the form of surgical resection and neoadjuvant therapy is considered the gold standard; however, these procedures are associated with significant postoperative morbidity and prolonged recovery times. Prehabilitation aims to combat this by physically and psychologically optimising patients preoperatively to handle the stress of surgery and improve postoperative outcomes.</p><p><strong>Aim: </strong>To evaluate the effectiveness of prehabilitation in patients undergoing gastric or oesophageal cancer resections.</p><p><strong>Methods: </strong>Standard medical databases such as MEDLINE, EMBASE, PubMed, and Cochrane Library were searched to find randomised, controlled trials comparing prehabilitation <i>vs</i> no-prehabilitation in patients undergoing gastric or oesophageal cancer resections. All data were analysed using Review Manager Software 5.4, and the meta-analysis was performed with a random-effect model analysis.</p><p><strong>Results: </strong>A total of 16 studies were included (<i>n</i> = 1479), recruiting adult patients undergoing gastric or oesophageal cancer resections. In the random effect model analysis, prehabilitation was associated with fewer postoperative complications compared to no prehabilitation (Odds ratio: 0.43, 95%CI: 0.31-0.58, <i>Z</i> = 25.28, <i>P</i> < 0.00001). Additionally, prehabilitation was associated with a lower postoperative readmission rate (risk ratio: 0.58, 95%CI: 0.35-0.96, <i>Z</i> = 2.10, <i>P</i> = 0.04) and a shorter length of stay [standardised mean difference (SMD): -0.19, 95%CI: -0.37 to -0.02, <i>Z</i> = 2.21, <i>P</i> = 0.03] compared to no-prehabilitation. Prehabilitation was also found to improve preoperative 6-minute walking distance (6-MWD) compared to no-prehabilitation (SMD: 0.72, 95%CI: 0.21-1.23, <i>Z</i> = 2.75, <i>P</i> = 0.006). No statistical difference was found in postoperative 6-MWD, mortality, and severe complications.</p><p><strong>Conclusion: </strong>Prehabilitation was found to be effective in reducing postoperative morbidity and improving preoperative physical health in patients undergoing gastric or oesophageal cancer resections.</p>","PeriodicalId":23953,"journal":{"name":"World Journal of Gastrointestinal Endoscopy","volume":"17 9","pages":"109033"},"PeriodicalIF":1.8000,"publicationDate":"2025-09-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12444260/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4253/wjge.v17.i9.109033","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Gastric and oesophageal cancers are among the leading causes of cancer-related mortality globally. Treatment in the form of surgical resection and neoadjuvant therapy is considered the gold standard; however, these procedures are associated with significant postoperative morbidity and prolonged recovery times. Prehabilitation aims to combat this by physically and psychologically optimising patients preoperatively to handle the stress of surgery and improve postoperative outcomes.
Aim: To evaluate the effectiveness of prehabilitation in patients undergoing gastric or oesophageal cancer resections.
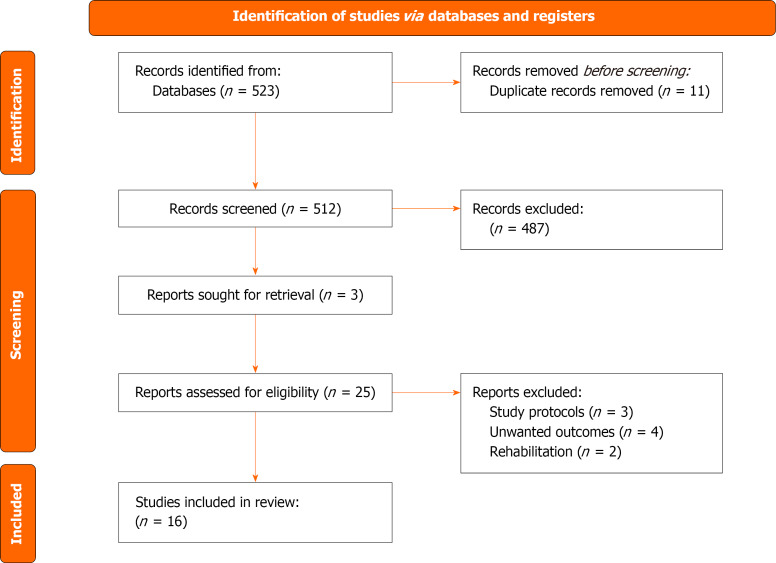
Methods: Standard medical databases such as MEDLINE, EMBASE, PubMed, and Cochrane Library were searched to find randomised, controlled trials comparing prehabilitation vs no-prehabilitation in patients undergoing gastric or oesophageal cancer resections. All data were analysed using Review Manager Software 5.4, and the meta-analysis was performed with a random-effect model analysis.
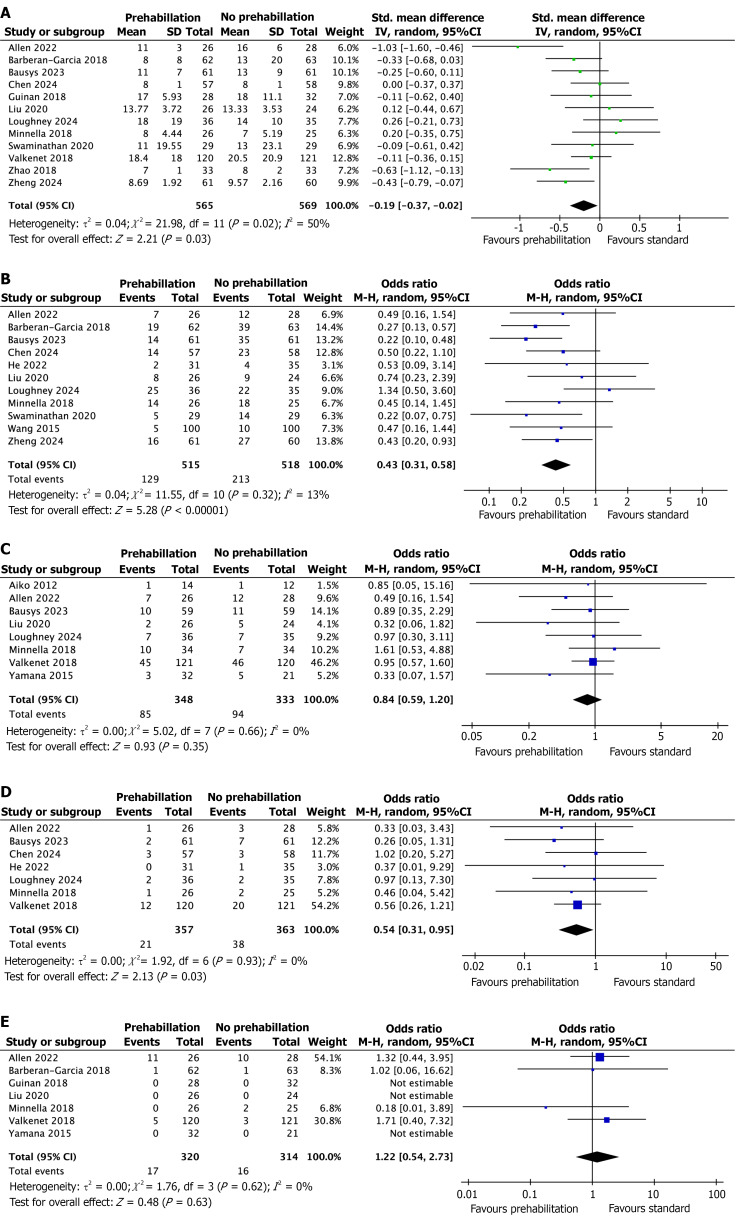
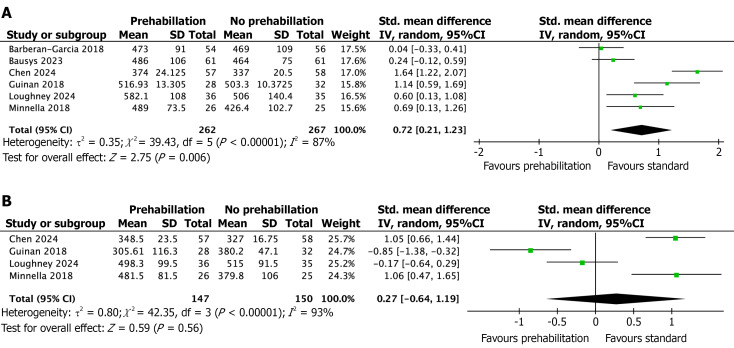
Results: A total of 16 studies were included (n = 1479), recruiting adult patients undergoing gastric or oesophageal cancer resections. In the random effect model analysis, prehabilitation was associated with fewer postoperative complications compared to no prehabilitation (Odds ratio: 0.43, 95%CI: 0.31-0.58, Z = 25.28, P < 0.00001). Additionally, prehabilitation was associated with a lower postoperative readmission rate (risk ratio: 0.58, 95%CI: 0.35-0.96, Z = 2.10, P = 0.04) and a shorter length of stay [standardised mean difference (SMD): -0.19, 95%CI: -0.37 to -0.02, Z = 2.21, P = 0.03] compared to no-prehabilitation. Prehabilitation was also found to improve preoperative 6-minute walking distance (6-MWD) compared to no-prehabilitation (SMD: 0.72, 95%CI: 0.21-1.23, Z = 2.75, P = 0.006). No statistical difference was found in postoperative 6-MWD, mortality, and severe complications.
Conclusion: Prehabilitation was found to be effective in reducing postoperative morbidity and improving preoperative physical health in patients undergoing gastric or oesophageal cancer resections.
背景:胃癌和食管癌是全球癌症相关死亡的主要原因之一。手术切除和新辅助治疗被认为是金标准;然而,这些手术有明显的术后发病率和较长的恢复时间。预康复旨在通过术前优化患者的生理和心理来应对手术压力并改善术后结果。目的:评价胃癌、食管癌切除术患者的康复效果。方法:检索MEDLINE、EMBASE、PubMed和Cochrane图书馆等标准医学数据库,查找比较胃癌或食管癌切除术患者预康复与非预康复的随机对照试验。所有资料采用Review Manager软件5.4进行分析,采用随机效应模型分析进行meta分析。结果:共纳入16项研究(n = 1479),招募接受胃癌或食管癌切除术的成年患者。在随机效应模型分析中,预训练与未预训练相比,术后并发症较少(优势比:0.43,95%CI: 0.31-0.58, Z = 25.28, P < 0.00001)。此外,与不进行预适应相比,预适应具有较低的术后再入院率(风险比:0.58,95%CI: 0.35-0.96, Z = 2.10, P = 0.04)和较短的住院时间[标准化平均差(SMD): -0.19, 95%CI: -0.37至-0.02,Z = 2.21, P = 0.03]。与未进行预训练相比,预训练可改善术前6分钟步行距离(SMD: 0.72, 95%CI: 0.21-1.23, Z = 2.75, P = 0.006)。术后6-MWD、死亡率、严重并发症无统计学差异。结论:术前康复对降低胃癌或食管癌切除术患者的术后发病率和改善术前身体健康状况有较好的效果。
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


